Localization: Proximal femur, pelvis, proximal humerus, scapula, and proximal tibia. In long bones, it starts metaphyseal extending as far as half or more of the entire bone.
Clinical: Deep, discontinuous, mild pain with small swelling. In the pelvis and at more advanced phases, large soft tissue mass is present. Pathologic fractures rare.
Imaging: On x-ray – intraosseous, osteolytic, geographic lesion with diffused, irregular, granules, nodules, and radiopaque rings of calcifications. Sometimes, a bubbling or “honeycomb” feature, metallic, or compact opacity. Cortex is scalloped, thinned, and destroyed. Often, it is thickened because the cortical bone reacts to the slow neoplastic infiltration with hyperostosis. Periosteal reaction is faint, with short perpendicular spiculae as a velvet or “beard” appearance. Margins may be sharp, with partial sclerotic rim or ill-defined, faded. It grows where there is less resistance (along the medullary canal). Soft tissue mass are not calcified. On bone scan – increased uptake more than radiographic extension. On angiography – avascular, but there may be a peripheral vascularization around the mass. On CT – typical calcified radiolucency, endosteal scalloping, buttressing, no enhancement, and often well contained. May show remnants of prior enchondroma. On MRI – gray homogeneous signal contrasts clearly with white marrow signal on T1, typical bright lesion on T2, and unexpected medullary extension on coronal projection.
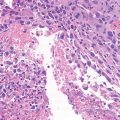
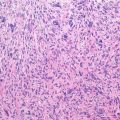
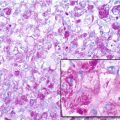
Histopathology: Lobular, faceted mass of grayer, softer, juicer, more transparent than normal cartilage. Frequent gelatinous, grayish white, mucoid, hemorrhagic, and necrotic areas. Spots or calcified rings to the periphery of the lobules, hard and gritty, with a chalky yellowish aspect. Grade 1–20 %, well-differentiated in cartilage. Slightly larger nuclei, rounded nuclei of different size, mitotic figure absent, frequent cells with double nuclei, more frequent calcifications, and infiltrating surrounding bony trabeculae. Grade 2–60 %, hypercellular lesion with hyperchromatic nuclei, frequent binucleate cells, myxoid areas with spindle-stellate cells gathered in short cords or little groups spread in abundant, semi-liquid, ground substance, extensive infiltration of the medullary spaces, thin pseudocapsule with neoplastic satellites. Grade 3–20 %, high cellularity with pleomorphic, hyperchromatic, gigantic, bizarre, with three or more nuclei. Mitotic figures. Diffusely infiltrating the bone marrow spaces with destruction of bony trabeculae and the soft tissue. Solid intravenous plugs.
Course and Staging: Very slow growth. Typical progression in malignancy: transformation from a low to high grade or to another malignant tumor. Grade 1: very rare metastases, recurrence even after 10 years. Grade 2: frequent early or late metastases, recurrence within 5 years. Grade 3: higher rate of early metastases, recurrence often within 1 year, usually stage IIB.
Treatment and Prognosis: Wide or radical resections are curative. High risk of recurrence with inadequate margins and when incisional biopsy is not performed carefully because tumoral cells may be implanted in the soft tissue. Lung metastases must be excised. Radio- and chemotherapy are not used because they are poorly effective. Death is rare in grade 1 lesions, but it occurs in 30 % and 60 %, respectively, of grade 2 and 3 lesions.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


