Chapter 9 Scrotum
Barbara Pawley and Adrian Dawkins
9 Questions and Answers
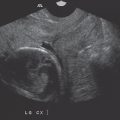
Question 9.1: In the transverse view of the testis, what does the yellow arrow indicate?

Convergence of the seminiferous tubules.
Reverberation artifact.
Focal scarring from prior infection.
Tunica vaginalis.
Answer:
A. Correct. The yellow arrow indicates the mediastinum testis, representing the point at which the seminiferous tubules converge.
B. Incorrect. Reverberation artifact is seen as a series of equally spaced parallel lines due to multiple reflections of sound between two closely spaced structures.
C. Incorrect. The mediastinum testis is a normal anatomic structure and not the result of scarring.
D. Incorrect. The tunica vaginalis is not invested into the parenchyma of the testis.
Question 9.2: Which of the following statements is correct? The tunica vaginalis______.
Is a single layer.
Is deep to the tunica albuginea.
Is a mesothelium-lined sac.
None of the above.
Answer:
C. Correct. The tunica vaginalis is a mesothelium-lined sac. Consequently, lesions of mesothelial origin may occur, manifesting as extratesticular masses. Such lesions include adenomatoid tumor and mesothelioma.
A. Incorrect. The tunica vaginalis forms two layers, the parietal and visceral layers. These are splayed in the setting of a hydrocele.
B. Incorrect. The layers of the tunica vaginalis are superficial to the tunica albuginea. The tunica albuginea is a fibrous layer that closely invests the testis.
D. Incorrect.
Question 9.3: This patient was evaluated for a possible inguinal hernia. The yellow arrowhead indicates the right epididymis. The left epididymis demonstrated a similar appearance. What is the most likely explanation?

Epididymitis.
Torsion.
Right renal mass.
Vasectomy.
Answer:
D. Correct. The epididymis in enlarged and demonstrates a speckled appearance. This has been described as tubular ectasia of the epididymis and is a frequent finding in patients who have undergone a vasectomy.
A. Incorrect. There is no supportive evidence to suggest acute inflammation of the testis and/or epididymis as there is no demonstrated hypervascularity.
B. Incorrect. There is no supportive evidence to suggest testicular torsion.
C. Incorrect. A right renal mass, with venous invasion, may lead to a right varicocele due to obstruction of the right testicular vein. However, a varicocele was not imaged.
Question 9.4: A patient with a prior history of a vasectomy presents with a lump within the right hemiscrotum, superior to and separate from the testis. What is the likely diagnosis?

Abscess.
Epidermoid cyst.
Adenomatoid tumor.
Sperm cell granuloma.
Answer:
D. Correct. The image demonstrates a solid rounded well-defined mass. While the imaging appearances are somewhat nonspecific, the history of a prior vasectomy coupled with the location make a sperm cell granuloma the likely diagnosis. A sperm cell granuloma forms from chronic inflammation in response to a prior vasectomy and tends to occur with the epididymis or along the vasa deferentia.
A. Incorrect. An abscess presents as a complex fluid collection with surround hypervascularity.
B. Incorrect. An epidermoid cyst is typically an intratesticular lesion.
C. Incorrect. An adenomatoid tumor is the most common extratesticular tumor and is typically solid and well defined. It is certainly a worthy differential consideration for this finding, however the history of a prior vasectomy renders this a less likely choice.
Question 9.5: This patient was evaluated for a scrotal mass. The tubular structure being measured was confirmed to be a vessel with Doppler imaging. Which statement is correct?

This finding is more frequent on the right.
The caliber of the vessel is within normal limits.
Apparent echogenic material within the vessel is due to thrombus.
The finding may result in subfertility.
Answer:
D. Correct. The image demonstrates dilated vessels within the hemiscrotum. This is the classic appearance of a varicocele, dilation of the pampiniform venous plexus above 3 mm. This typically results from reversal of flow within the testicular vein and is much more common on the left, presumably due to the horizontal course of the left renal vein, into which the left testicular vein drains. The Valsalva maneuver results in an exacerbation of the findings due to reflux. Patients with varicoceles may develop subfertility due to impaired spermatogenesis in part due to the increased local temperature caused by dilated veins.
A, B—Incorrect. Refer to the explanation of the correct choice above.
C. Incorrect. The apparent echogenic material within the vein is artifactual secondary to slow flow.
Question 9.6: A 10-year-old boy presents with left testicular pain. A scrotal ultrasound is obtained, an image from which is demonstrated below. What is the likely diagnosis?

Orchitis.
Epididymitis.
Left testicular torsion.
Germ cell tumor.
Answer:
A. Correct. The image demonstrates a swollen left testis with increase vascular flow, the typical appearance of acute orchitis.
B. Incorrect. While epididymitis frequently occurs in conjunction with orchitis, the left epididymis is not imaged. Therefore, epididymitis cannot be confirmed on the current images.
C. Incorrect. Decreased vascular flow is expected within the affected testes in cases of acute torsion.
D. Incorrect. A discrete testicular mass is not imaged.
Question 9.7: After 2 weeks of treatment, a patient with acute orchitis returns for a follow-up ultrasound. Which statement best describes this new appearance?

There has been inadequate treatment of underlying infection.
The testis is now devitalized secondary to progression of intermittent torsion.
An enlarging hematoma is present.
There has been progression of aggressive neoplasm.
Answer:
A. Correct. The image demonstrates suppurative material exuding from the left testes, beyond the tunica albuginea. The findings are consistent with rupture of an intratesticular abscess, leading to a pyocele. This occurred secondary to inadequate antibiotic treatment of orchitis.
B. Incorrect. Established torsion would manifest as heterogeneity of the testicular parenchyma and an absence of vascular flow.
C. Incorrect. A hematoma is not present.
D. Incorrect. An underlying neoplasm is not present.
Question 9.8: A 28-year-old male presents with a painless testicular lump. A scrotal ultrasound was performed, an image from which is presented here. Which statement is correct?

This finding is most frequently associated with microlithiasis.
This lesion is almost certainly benign.
An orchiectomy is the most appropriate treatment.
A course of antibiotics would be appropriate.
Answer:
B. Correct. The image demonstrates a well-defined, rounded intratesticular lesion within a lamellated or “onion-skin” appearance. These finding are typical of an epidermoid cyst, a benign lesion.
A. Incorrect. The epidermoid cyst is not associated with microlithiasis.
C. Incorrect. This lesion may be enucleated, sparing the testis.
D. Incorrect. A course of antibiotics is not indicated.
Question 9.9: An 18-year-old male straddles a wooden fence. He presents 2 weeks later with scrotal swelling and undergoes an ultrasound. The testes are normal. Given the finding below, what management strategy is appropriate?

Administration of antibiotics.
Obtain a pelvic radiograph.
Local incision.
None of the above.
Answer:
C. Correct. The image demonstrates a slender echogenic line within a surrounding well-defined hypoechoic focus situated within the edematous scrotal skin. This finding is consistent with a retained wooden splinter with a surrounding “foreign body granuloma.” A local incision, especially if guided by sonographic marking, would facilitate retrieval.
A. Incorrect. Antibiotics would not provide definitive treatment for this condition.
B. Incorrect. A pelvic radiograph is unnecessary especially since wooden foreign bodies are often radiolucent.
D. Incorrect.
Question 9.10: A diabetic patient presents with groin pain and undergoes a scrotal ultrasound. Which statement is true regarding the finding below?

The scrotal skin demonstrates coarse calcification.
A retained foreign body is present.
Steroid administration is required.
None of the above.
Answer:
D. Correct. The image demonstrates gas within thickened scrotal skin, the hallmark of Fournier’s gangrene. This life-threatening condition is most prevalent in middle-aged males, with diabetes being a predisposing factor. Urgent debridement and broad-spectrum antibiotics are required for an optimal outcome.
A. Incorrect. The echogenic foci within the scrotal skin demonstrate the classic “dirty shadowing” consistent with gas as opposed to calcification.
B. Incorrect. A retained foreign body is not imaged.
C. Incorrect. Steroids are not indicated.
Question 9.11: These sonographic images were obtained in a 46-year-old male with testicular pain. Of the options below, which best accounts for the findings?

Ectasia of the rete testis and left spermatoceles.
Ectasia of the rete testis and left complex hydrocele.
Intratesticular varicocele and left spermatoceles.
Intratesticular varicocele and left complex hydrocele.
Answer:
A. Correct. The images demonstrate tubular cystic areas along the mediastinum testis, consistent with tubular ectasia of the rete testes. This is typically observed in middle-aged men and felt to be secondary to obstruction of the vasa efferentia, (the communicating tubular network between the rete testis and epididymal head). The condition is often bilateral though asymmetric. In the case presented, it is more marked on the right. Tubular ectasia of the rete testis is frequently associated with spermatoceles, a type of extratesticular cyst. Several spermatoceles are noted along the left testis.
B. Incorrect. A hydrocele occurs within the tunical space and typically surrounds the testis.
C. Incorrect. An intratesticular varicocele may create an appearance similar to tubular ectasia. However, the presence of vascular flow on Doppler imaging within an intratesticular varicocele and the classic location of tubular ectasia allow sonographic differentiation of these two entities.
D. Incorrect. A varicocele and hydrocele are not present.
Question 9.12 A 62-year-old male presents with testicular pain and undergoes a testicular ultrasound. Representative images are presented below. What is the most likely diagnosis?

Seminoma.
Embryonal tumor.
Hematoma.
Lymphoma.
Answer:
D. Correct. The images demonstrate a well-defined hypoechoic mass with the testis. The mass is also avidly hypervascular. These findings, coupled with the patient’s age, make lymphoma the most likely diagnosis. Testicular lymphoma is most often of the B cell variety.
A. Incorrect. Seminomas are the most common testicular tumor but typically occur in a younger demographic (average age of 40 years).
B. Incorrect. The sonographic features of this tumor are nonspecific but again, embryonal testicular tumor tends to occur in younger patients (25–35 years).
C. Incorrect. A hematoma is unlikely to show internal vascular flow.
Question 9.13: Regarding the image below which statement is correct?

The lesion is most likely a Sertoli cell tumor.
The ipsilateral groin should be evaluated to excluded lymphatic spread since this is the first site of nodal disease.
Both of the above.
None of the above.
Answer:
D. Correct. The image demonstrates multiple tiny punctate echogenic foci throughout the testicular parenchyma, consistent with testicular microlithiasis. Testicular microlithiasis has been associated with the development of testicular tumors, in particular germ cell tumors such as seminomas. Testicular tumors first metastasize to paracaval lymph nodes consistent with lymphatic drainage.
A, B—Incorrect. Testicular tumors first metastasize to paracaval lymph nodes consistent with lymphatic drainage.
C. Incorrect.
Question 9.14: The image in (Question 9.13) demonstrates multiple tiny punctate echogenic foci throughout the testicular parenchyma, consistent with testicular microlithiasis. All the following are associated with the condition except?
Klinefelter syndrome.
Trisomy 21.
Alveolar proteinosis.
Klippel–Trenaunay syndrome.
Answer:
D. Correct. Klippel-Trenaunay syndrome is not associated with testicular microlithiasis.
A. Incorrect. Klinefelter syndrome is associated with testicular microlithiasis.
B. Incorrect. Trisomy 21 is associated with testicular microlithiasis.
C. Incorrect. Alveolar proteinosis is associated with testicular microlithiasis.
Question 9.15: A 26-year-old male presents with groin pain for which he undergoes a scrotal ultrasound. A representative image is demonstrated below. How should this finding be managed?

Orchiectomy.
Incision and drainage.
No intervention is necessary.
None of the above.
Answer:
C. Correct. The image demonstrates a well-defined anechoic intraparenchymal testicular cyst. These incidentally discovered lesions have no malignant potential and warrant no intervention.
A, B—Incorrect. No intervention is required.
D. Incorrect.
Question 9.16: A 17-year-old male presents with left testicular pain. He undergoes a scrotal ultrasound. Based on the images below, which statement is correct?

There is fairly symmetric vascular flow on color Doppler, effectively excluding testicular torsion.
The heterogenous mass at the upper aspect of the left testis is unlikely to represent a malignancy.
Both statements are correct.
Neither of the statements is correct.
Answer:
B. Correct. Intrascrotal, extratesticular masses are typically benign. The red arrow indicates a mass-like lesion at the superior aspect of the left testis. This demonstrates tubular internal contents and actually represents a “torsed” spermatic cord. It is to be remembered that testicular torsion is not actually twisting of the testis but rather twisting of the spermatic cord. For this reason, on clinical evaluation, the testis is not only tender, but also somewhat high-riding and more horizontal in lie. Consequently, the “exclude torsion” scanning protocol should always include an evaluation of the spermatic cord.
A. Incorrect. The subjective assessment of symmetric vascular flow is not sufficient to exclude testicular torsion. Instead, the absent or markedly decreased vascular flow within one testis may help support the diagnosis of torsion.
C, D—Incorrect.
Question 9.17: A 21-year-old patient presents with a roughly 2-week history of on and offscrotal pain. A scrotal ultrasound is performed. The images are consistent with which of the following conditions?

Right orchitis.
Left testicular neoplasm.
Left testicular infarction.
None of the above.
Answer:
C. Correct. The image demonstrates thickening of the scrotal skin and absent vascular flow within the heterogenous left testis. The findings are consistent with an infarcted left testis, secondary to torsion.
A. Incorrect. The vascular flow and parenchymal pattern of the right testis are within normal limits. There is typically increased vascular flow in the setting of orchitis.
B. Incorrect. Though there is heterogeneity throughout the left testicular parenchyma, a discrete mass in not identified making an underlying neoplasm unlikely.
D. Incorrect.
Question 9.18: A 21-year-old male presents with right groin pain. A scrotal ultrasound is performed. Based on the images below, which statement is correct?

The right testis is normal but the left testis is likely to be congenitally absent.
The right testis is normal. An inguinal hernia is probably obscuring the left testis.
Both kidneys should be evaluated since there is a high likelihood of associated renal agenesis.
The ipsilateral groin and spermatic cord should be sonographically evaluated.
Answer:
D. Correct. In the setting of an incidentally discovered “absent testis,” an undescended testis/cryptorchidism should be excluded. Usually, the undescended testis is located within the ipsilateral groin and hence frequently amenable to sonographic visualization.
A. Incorrect. Undescended testis is much more likely than congenital absence of the testis.
B. Incorrect. In the setting of an intrascrotal inguinal hernia, the testis is still usually visible, albeit often displaced inferiorly within the scrotum.
C. Incorrect. There is no strong correlation between undescended testis and renal agenesis.
Question 9.19: A 21-year-old male undergoes a scrotal ultrasound. The left testis is not visualized within the left hemiscrotum. The left groin is imaged and the key finding depicted in the image below. Which statement is correct?

The structure being measured is consistent with a groin lymph node.
There is a 30- to 50-fold increased risk of malignancy.
A biopsy is warranted.
If an underlying tumor develops, it would most likely be a Sertoli cell tumor.
Answer:
B. Correct. Undescended testis/cryptorchidism is associated with a 30- to 50-fold increased risk of malignancy, with seminoma and embryonal cell carcinoma accounting for the majority of cases.
A. Incorrect. Though a normal lymph node may be hypoechoic and oval in shape, the absence of the typical “echogenic hilum” allows the two entities to be distinguished.
C. Incorrect. If there are sufficient associated suspicious features, such as microlithiasis, an orchiectomy is indicated.
D. Incorrect. Seminoma and embryonal cell carcinoma account for the majority of malignancies in the setting of cryptorchidism.
Question 9.20: Images of the bilateral testes of a 34 year-old male are presented. The images demonstrate bilateral testicular masses. Which statement is correct with respect to bilateral testicular tumors?

Synchronous tumors are more frequently encountered than metachronous tumors.
A testicular metastasis is more likely to arise from a contralateral testicular primary than from a distant primary.
Testicular lymphoma is bilateral in roughly 30% of cases.
None of the above.
Answer:
C. Correct. Testicular lymphoma is bilateral in up to 30% of cases.
A. Incorrect. Synchronous testicular tumors are much less common than metachronous tumors, with synchronous tumors accounting for only 10% of bilateral testicular tumors.
B. Incorrect. The testes do no share vascular and lymphatic connections, so a tumor in one testis is unlikely to spread to the other. Instead testicular metastases, though rare, likely arise from other primary sources such as the prostate.
D. Incorrect.
Question 9.21: Images of the bilateral testes of a 34 year-old male are presented. The images demonstrate bilateral testicular masses. Imaging of the upper abdomen of the patient revealed bilateral adrenal masses. What is the most appropriate management of this condition?

Percutaneous biopsy of the adrenal lesions.
Colonoscopy.
Chemotherapy and scrotal radiotherapy.
High-dose glucocorticoid therapy.
Answer:
D. Correct. The patient’s testicular masses are adrenal rest tumors. Testicular adrenal rests are clusters of cells that become trapped within the developing gonad. These adrenal rests can be found in roughly 10% of newborns and about 2% of adults. They are typically asymptomatic, unless exposed to elevated levels of adrenocorticotropic hormone, in which case they enlarge to form masses. This patient has a history of congenital adrenal hyperplasia which led to stimulation of the adrenal rest. This condition may be treated with steroids.
A, B, C—Incorrect. These are not indicated.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


