Fig. 1
Interstitial involvement in a child of 12 months with viral infection. a Chest radiograph shows an enlarged right hilum, with linear images. b Interstitial nodular pattern in a 17-year-old boy with CMV infection after BM transplant
When the pneumonia is severe, the pattern shows a diffuse, bilateral, sharply defined reticular (stringy) or nodular infiltrate (Fig. 1b). There is no air bronchogram and associated pleural effusion.
Alveolar (airspace) disease is characterized by a plethora of descriptive names. The typical alveolar infiltrate is a smooth, homogeneous increase in density (whiteness) of the lungs (Fig. 2). The most common alveolar infiltrate is well-defined, dense homogeneous lobar or segmental consolidation, with an air bronchogram within it. There is commonly associated pleural effusion.
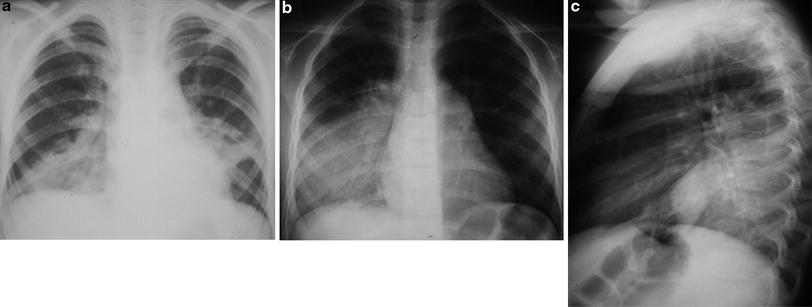
Fig. 2
Alveolar pattern on chest radiograph in a 10-year-old child with pneumococcal pneumonia. a Heterogeneous opacity with ill-defined boundaries air bronchogram in the right base and lower third of the left lung field. b and c Another similar case with alveolar pattern in a 11-year-old child with lobar pneumococcal pneumonia
Mixed infiltrates, not surprisingly, have features of both alveolar and interstitial patterns. If an unknown pulmonary infiltrate cannot comfortably be classified as either alveolar or interstitial, it is considered to have the mixed pattern (Fig. 3). The prototype of a mixed infiltrate is an ill-defined area of mildly increased density containing finely dilated air bronchioles. There is usually no significant pleural effusion.

Fig. 3
Mixed infiltrate on a chest radiograph in an 8-year-old girl with streptococus pneumonia. There is an ill-defined area of mildly increased density (containing finely dilated air bronchioles). There is usually no significant pleural effusion
2.4 Evaluation of Children with Pneumonia
Pulmonary infection is the most common indication for performing chest radiography. It is the radiological imaging that confirms the diagnosis and allows evaluating the location and extent of infection.
The common difficulties in the etiologic diagnosis of pneumonia led pediatricians and radiologists to a need to specify the causative infectious agents based on radiological patterns.
In this respect, special importance was placed on the distinction between viral and bacterial pneumonias, attributing to the viral disease interstitial pattern and the bacterial infection involving airspace.
Although providing evidence suggestive of the causative agent, the chest radiograph cannot confirm viral infection nor confirm or eliminate bacterial etiology. In fact, in infancy, pneumonia usually produces a combination of changing the airspace and interstitium. However, some aspects may be useful in distinguishing between viral and bacterial pneumonia.
The roles of imaging in the evaluation of immunocompetent children with Community-acquired pneumonia are multiple: confirmation or exclusion of pneumonia, characterization and prediction of infectious agents, exclusion of other symptoms, evaluation when there is failure to resolve, and evaluation of all related complications (Donnelly and Klosterman 1997a).
Concerning characterization and prediction of infectious agents, the previously described patterns of radiographic and CT findings which suggest a specific infectious agent are rarely of clinical relevance in the previously healthy child who is imaged for suspected pneumonia (Donnelly 2002).
Cough and fever are two of the most common symptoms of illness in the pediatric age group and suggest respiratory pathogenesis, particularly pneumonia. Radiographic findings in combination with clinical evaluation are vital in deciding whether treatment with antibiotics or further study is indicated. The character of pneumonia that it is revealed radiographically, in combination with the clinical pattern of the disease, assists the physician in deciding whether antibiotics are indicated. Despite numerous advances in pediatric care and imaging modalities, the plain chest radiography remains the most valuable tool available for evaluating airway and the lungs and for assessing the site and gross character of pulmonary disease (Wesenberg et al. 2006).
In considering the multiple entities that cause cough and fever in the pediatric age groups, two approaches to the differential diagnosis are available.
The first is based on the clinical character of symptoms, specifically acute illness versus illness that is chronic or recurrent.
The second approach is based on the age of the patient, because there are distinct age predilections of agents that cause cough and fever in children.
2.5 Differential Diagnosis According to Clinical Character of Illness and Age of Patient
The three main causes of community-acquired pneumonia (CAPs) in pediatric patients are viral, atypical, and bacterial.
As a group, viruses account for approximately 65 % of all pneumonias that occur in pediatric patients. Respiratory syncytial virus (RSV) is the responsible organism in approximately 50 % of the cases.
The epidemic and seasonal occurrence of pneumonias and lower tract infections is a well-known phenomenon. RSV and metapneumovirus are responsible for yearly outbreaks, during winter.
The respiratory viruses, as a group, account for approximately 90 % of the agents recovered from children younger than 4 years of age (Wesenberg et al. 2006).
The most common specific agent that produces demonstrable pneumonia in pediatric age group is mycoplasma pneumonia, the most prevalent in school-age children. It is one of the main causes of atypical pneumonia. In children younger than 4 years of age, the incidence drops to approximately 5 %.
The most common cause of other bacterial pneumonia in pediatric age group is Streptococcus pneumonia. In addition, there has been a recent increase in the prevalence of pneumonias caused by community-acquired methicillin–resistant staphyllococcus aureus (MRSA). Less common causative bacteria are S. pyogenes, Klebsiella species, and gram-negative organisms (Wesenberg et al. 2006).
2.6 Viral Pneumonias
Viral pneumonia usually originates interstitial dispersed patterns, sometimes bilateral. They are frequently ill-defined opacities, involving one or more lobes, being located mainly in the perihilar regions. There is often thickening of the bronchial wall and densities and peribronchial opacities scattered non-confluent and areas of atelectasis affecting predominantly the upper lobes and middle lobe.
Often the small airways are involved causing anterior prolapse with hypersuflation of the lungs, prolapsed of the sternum, and lowering the of diaphragm.
The most common radiographic findings are bilateral, symmetrical, parahilar, and bronchial opacities with or without atelectasis and air trapping (Fig. 4). Focal and asymmetrical disease is not uncommon. Lymph node enlargement can occur, but pleural effusion is rare (Daltro et al. 2011).
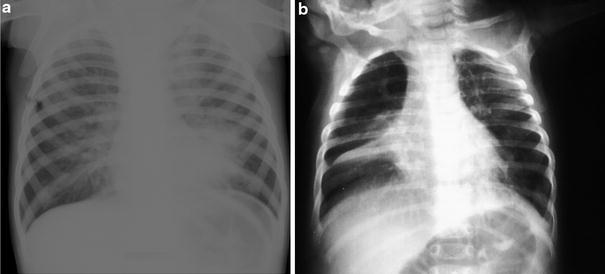
Fig. 4
Viral infection in a 22-month-old boy with fever and increased respiratory distress. a Radiography of the 4th day of hospitalization shows exuberant bilateral interstitial pattern. Serology revealed adenovirus infection. b Another similar case in a 12-month-old child with RSV infection. Atelectasis of the middle lobe is also shown
Recently, viral infection has been recognized as a cause of severe pneumonias leading to respiratory failure and death. Higher mortality rates are associated to coronavirus A (SARS, severe acute respiratory syndrome), and influenza virus type A H5N1 (bird flu) and type A H1N1. As with other viral pneumonias, focal or diffuse interstitial opacities are the initial chest radiograph presentation, but they can progress rapidly to bilateral areas of consolidation (Daltro et al. 2011).
The radiographic findings in RSV bronchiolitis are predominantly those of hyperaeration of the lungs with a variable degree of perihilar interstitial infiltrate. Usually the lungs are clear peripherally. Typically the bilateral, perihilar interstitial infiltrate is suggestive of mild to moderate hilar enlargement that it is indistinct on both projections. A more widespread interstitial infiltrate occurs in more severe infections, and areas of subsegmental atelectasis are common, reflecting mucous plugging.
The lungs in pneumonia commonly are also hyperaerated but generally less so than in RSV bronchiolitis. Radiographic clearing is not as rapid as clinical recovery, and complete clearing may take as long as 2–5 months.
The initial radiographic findings in adenoviral pneumonia are nonspecific and are shared with the other viral pneumonias. The most common manifestation is bilateral, perihilar interstitial infiltrate.
The pulmonary sequelae of adenovirus pneumonia are usually evident on follow-up controls (Fig. 5). A mild form of adenoviral pneumonia is chronic pneumonitis, with associated fibrosis and mild bronchiectasis. In severe disease, necrotizing bronchiolitis progress to obliterative bronchiolitis, which leads to unilateral hyper lucent lung (Swyer-James syndrome) or bilateral hyperlucent lung, with or without areas of associated bronchiectasis and chronic atelectasis.
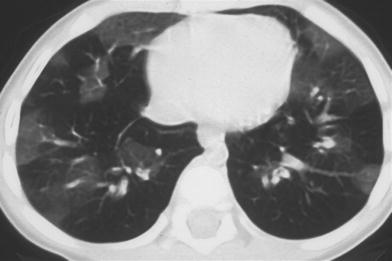
Fig. 5
Obliterative Bronchiolitis as sequelae of adenovirus pneumonia in an 8-year-old girl. Follow-up CT image shows a mosaic pattern with some patchy air-trapping areas and a normal expiratory ground-glass areas
2.7 Atypical Pneumonia
A wide variety of infectious agents (virus and bacteria) may be the cause of atypical pneumonia. Atypical features in pneumonia include prominent extrapulmonary features (e.g., headache, sore throat, and pharyngeal exudates), minimal or disparate chest signs on physical examination, subacute onset, non focal lung opacity on chest radiographs, lack of clinical response to antibiotics, lack of substantial leukocytosis, and a slow disease course. On chest radiographs, the pulmonary opacity is seen as either airspace, reticular (linear), or band-like opacities in a non focal, patchy, or mottled distribution, with various degrees of density, usually without a single dense area of consolidation (Hedieh et al. 2011).
The most specific agent that produces demonstrable pneumonia in the pediatric age group is a bacterium, Mycoplasma pneumoniae, most prevalent in school-age children.
The radiographic pattern produced by M. pneumoniae is most commonly an ill-defined, mildly increased density segmental or lobar consolidation with involvement that is usually in the lower lobes. Acutely, a perihilar interstitial pattern is present. Typically, there are areas bronchiolar and acinar dilatations, commonly within the consolidation, that suggest mild micro cyst formation. A patchy, alveolar bronchopneumonic pattern may occasionally be seen. There is usually no pleural effusion (Wesenberg et al. 2006).
In the mycoplasma pneumonia, radiological aspects are not specific. Often there are bronchopneumonic opacities mainly affecting the lower lobes. There may also be interstitial or peribronchial densities as well as segmental or subsegmental atelectasis. Pleural effusions are not uncommon and are usually minor and transient. Often there is discrepancy between the exuberant symptoms, the poor objective examination and marked radiographic lesions (Fig. 6).

Fig. 6
Mycoplasma pneumonia in a 11-year-old girl with cough and fever. Chest radiograph shows areas of hypotransparencies and lung densities in both lungs. Serology was positive for M. pneumoniae and antibiotic therapy instituted led to clinical and radiological resolution
Patients who have Chlamydia trachomatis pneumonia have a fairly typical bilateral, perihilar interstitial pattern of infiltrate. Patchy fluffy-appearing alveolar infiltrates are usually bilaterally superimposed on this pattern, and radiographic findings are often more severe than clinical symptoms.
Chlamydia pneumoniae causes an atypical pneumonia virtually indistinguishable from that caused by Mycoplasma (Wesenberg et al. 2006).
In C. trachomatis pneumonia, the chest radiograph often shows hyperinflation and diffuse interstitial or alveolar opacities.
There are also the aspects of clinical pneumonia (cough in infants 3 weeks to 4 months prior afebrile and conjunctivitis), the epidemiological context (mother gynecological infection in the last trimester of pregnancy), and the specific laboratory tests (hemogram with eosinophilia), which will lead us to the possible causing agent (Fig. 7).

Fig. 7
Newborn with conjunctivitis and polipneia, with abnormal pulmonary auscultation. Chest radiography showed a bilateral interstitial linear pattern and consolidation. Serology was positive for C. trachomatis and clinical evolution was favorable with antibiotics
2.8 Bacterial Pneumonias
Bacterial pneumonias account for only 3–5 % of all childhood pneumonias. In general, bacterial pneumonias have a sudden onset. The epidemic and seasonal occurrence of pneumonias and lower respiratory tract infections is a well-known phenomenon. A viral infection commonly precedes the bacterial pneumonia by several days to a week.
Radiologically, bacterial pneumonias usually cause dense lobar or segmental consolidation that frequently contains an air bronchogram. Patchy pneumonia is the second most common pattern. When present, findings that suggest bacterial rather than viral pneumonia include significant pleural effusion, abscess, and pneumatocele formation within pneumonic infiltrates.
The pattern of epidemic occurrence for school-age children (4–18 years) is distinctly different from that of preschool children.
The most common cause of other bacterial pneumonia in the pediatric age group is S. pneumoniae.
The bacterial pneumonia usually originates scattered opacities in infants, the segmental or lobar condensation is the most typical finding being located predominantly in the middle or at the periphery of the lung fields, especially when the agent is S. pneumoniae or Haemophilus influenzae (Fig. 8). Hilar engorgement is more common in pneumonia by H. influenzae or Staphylococcus aureus pneumonia, but can also occur in pneumococcal pneumonia. Pneumothorax or pleural effusion, including empyema, can occur particularly in staphylococcal infections and other purulent agents. Generally, the infection affects one lung but also can be bilateral (Fig. 9).
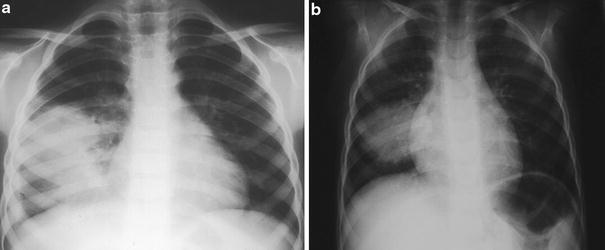
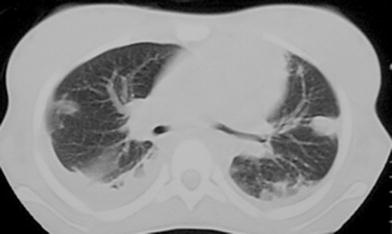
Fig. 8
Bacterial pneumonia in a 6-year-old boy with fever and thoracic pain. a The chest radiograph shows rounded opacity of the right lung and small lamellar spill along the right chest wall. A S. pneumonia was isolated. b Similar case of rounded pneumonia in a 7-year-old child with streptococcus infection
Fig. 9
Bacterial pneumonia in a 10-year-old girl, after cutaneous wound in the foot, developed fever and respiratory distress. Chest radiograph (not shown) and CT showed round opacities, and pleural fluid. A Staphilococcus aureus was isolated
Certain bacterial specimens originate necrotic foci in the parenchyma that communicate with the lumen of the airways, forming thin-walled and well-defined bubbles called pneumatoceles. In the course of pneumonia, an abscess can also arise, which differs from pneumatocel by presenting itself as an image with thick-walled cavitation that fades in the condensation surroundings, and often with liquid content (Fig. 10). Pneumotocels are more common in staphylococcal pneumonia, particularly in the convalescent phase, but other agents are also associated with bullous images, including Klebsiella pneumoniae, H. influenzae, S. pyogenes and S. pneumoniae. Sometimes bacterial pneumonia may present as spherical opacities (Fig. 8). Usually the edge of these pneumonias is not well-defined and the image does not look so round in two planes (PA and lateral). An X-ray follow-up days later often reveals a condensation without the initial round appearance.
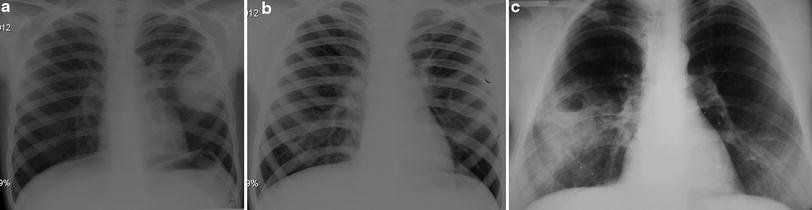
Fig. 10
Necrotic pneumonia in a 10-year-old boy with productive cough, fever and thoracic pain (a, b). a Chest radiograph revealed cavitated round opacity which evolved into pneumatocel after antibiotic theraphy. b A S. pneumonia was isolated. c Similar case of necrotic pneumonia in a 16-year-old boy with Stafilococcus aureus infection
Therefore, the presence of a segmental or lobar condensation, pleural effusion, necrotic foci, abscess, or pneumatocele in children with high fever and signs of toxicity suggest bacterial etiology.
S. pneumoniae pneumonia manifests as a dense, homogeneous, alveolar lobar, or segmental consolidation of lung parenchyma (Fig. 11). The consolidation begins in the peripheral air spaces and thus almost invariably abuts a pleural surface. The consolidation usually has an air bronchogram and middle well-defined border. Pleural effusion or empyema is common.

Fig. 11




S. pneumonia in a 45-day-old-girl, with fever, nasal obstruction, and respiratory distress. Chest radiograph showed bilateral opacities of the upper lobes. β-hemolytic Streptococcus was isolated in blood culture
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
