Location: Typically located in the long bone metaphysis, it can invade the epiphysis, especially in adults. Preferred sites proximal tibia (30 % of cases), small bones of the foot, and pelvis. Rare in the upper limb and in the trunk besides pelvis.
Clinical: Long-standing mild to moderate pain sometimes associated with bland local swelling is the typical scenario, because of the rather slow growth. Occasionally asymptomatic and discovered as incidental finding on roentgenograms.
Imaging: Small (generally <5 cm), metaphyseal, and eccentric radiolucent defect, usually with the long axis parallel to the bone of origin and occupying one half to two thirds of the diameter of the shaft; sometimes, especially in small bones, fusiform expansion of its entire contour. Sharply marginated by a lobulated shell of endosteal reactive bone because of a sclerotic rim. The cortex is usually canceled, with the tumor “bubbling out” into soft tissue. Little and peripheral periosteal reaction, chronic in nature and similar to that of periosteal chondroma. Intratumoral calcification is unusual. Isotope scan: moderately hot and corresponding to radiographic extent. CT: metaphyseal, eccentric, and subperiosteal, heavily marginated radiolucency, usually without any mineralization. MRI: homogenous intratumoral signal.
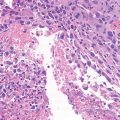
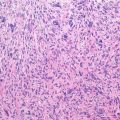
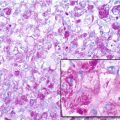
Histopathology: Gross: the tumor is rubbery soft, distinctly lobular, and clearly separated from the surrounding bone. Tissue is whitish or bluish and semitranslucent in chondromyxoid areas, tannish red in the undifferentiated and vascularized zones. Histology: lobular pattern better appreciated at low power, a light center, and a dark periphery. Basic elements stellate cells (blue) and myxoid background; center of lobule is hypocellular, periphery hypercellular. While the smaller lobules are exclusively or prevalently dark, the larger lobules are predominantly light, the dark part being limited to a narrow layer at the periphery of the lobules and in between them. These dark bands are absent where the lobules fuse together. Mitotic figures are not common. Cellular atypia may be present (15–20 % of cases). Occasionally, chondroblastoma-like cells at periphery.
Course and Stage: The tumor grows slowly and is generally small, at presentation usually stage 2 and occasionally stage 3. Few reports of malignant transformation.
Treatment: Aggressive curettage is usually indicated and frequently curative for either stage 2 and stage 3 tumors; recurrence rate probably lower than GCT and chondroblastoma. Consider en bloc resection for recurrent lesions and expendable bones.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


