24
Colorectal Cancer
Eugene C. Lin and Abass Alavi
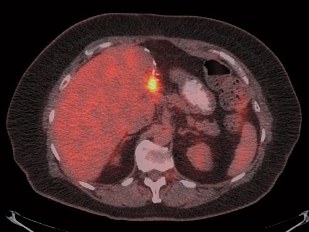
Positron emission tomography (PET) has no role in screening for colonic neoplasm, but colonic lesions may be detected incidentally on PET scans performed for other indications (Fig. 24.1).
- PET. Sensitivity 74%, specificity 84% for colonic neoplasm (adenomas or carcinoma) compared with colonoscopy.1
- If there is a known colon cancer, it will usually be detectable by PET. Tumor size and depth of invasion are associated with higher standardized uptake values (SUVs).2 One study suggests that PET is unlikely to miss a colon cancer,3 but another suggests that the sensitivity of PET for colon cancers < 2 cm is limited.4
- Lesion size. The detectability of colonic adenomas depends on lesion size. Other factors influencing detectability are shape (decreased sensitivity for flat morphology) and grade of dysplasia.3,4
- Seventy-two percent of adenomas > 11 mm in size are detected by PET.3
- Both adenomas (Fig. 24.1) and carcinomas (Fig. 24.2) may appear with increased uptake on PET. One study suggests that carcinomas generally have greater uptake than adenomas,5 but other studies suggest there is no difference in uptake.3,6
- Nonmalignant causes of uptake7
- Focal physiologic uptake can cause false-positive findings.
- With PET/CT, focal bowel uptake is false-positive approximately one third of the time.6,8 The false-positive rate is higher with PET alone.
- SUV values cannot distinguish between focal physiologic uptake and neoplasm.6,8
- Uptake in hyperplastic polyps has been described, although this is unusual.
- Hemorrhoids can have increased uptake likely secondary to inflammation.
- Uptake pattern. The pattern of uptake is helpful in differential diagnosis.
- Nodular colonic uptake is often due to a focal lesion.
- Segmental uptake is often secondary to inflammation.
- Diffuse uptake is usually normal. There is usually more uptake in the right colon, particularly in the cecum.9
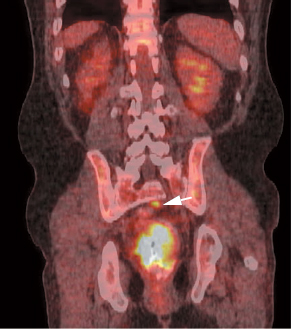
- Preoperative staging in colorectal cancer with PET is not commonly performed because patients will often undergo colectomy to relieve obstruction, and intraoperative staging can be done during surgery. PET is helpful in patients with a normal computed tomography (CT) scan and high carcinoembryonic antigen (CEA), where demonstration of metastatic disease may preclude surgery. In patients with advanced disease (Fig. 24.2), PET may allow optimal staging compared with findings during surgery.
- PET/CT colonography is more accurate in defining TNM (tumor-nodes-metastasis) stage than CT alone, primarily because of its more accurate definition of the T stage. The bowel distention during PET/CT colonography is helpful for evaluating the bowel wall and surrounding soft tissue. However, T stage is often of minor clinical relevance in colon cancer (accurate assessment of T stage preoperatively is more important in rectal cancer). Thus, the change in patient management from PET/CT in colorectal cancer staging is often due to detection of synchronous tumors.10
- Rectal cancer. PET may have value in advanced primary rectal cancer, particularly if neoadjuvant chemoradiation is being considered. In these patients it can detect distant metastatic or synchronous disease and upstage disease in 8 to 24% of patients.11–13
- Discordant findings (usually lymph node metastases) between PET/CT and CT are more common in low rectal cancers than in mid or high rectal cancers; therefore, PET/CT will more frequently add staging information in low rectal cancers.14
PET is a standard modality for evaluating colon cancer recurrence. The primary uses are
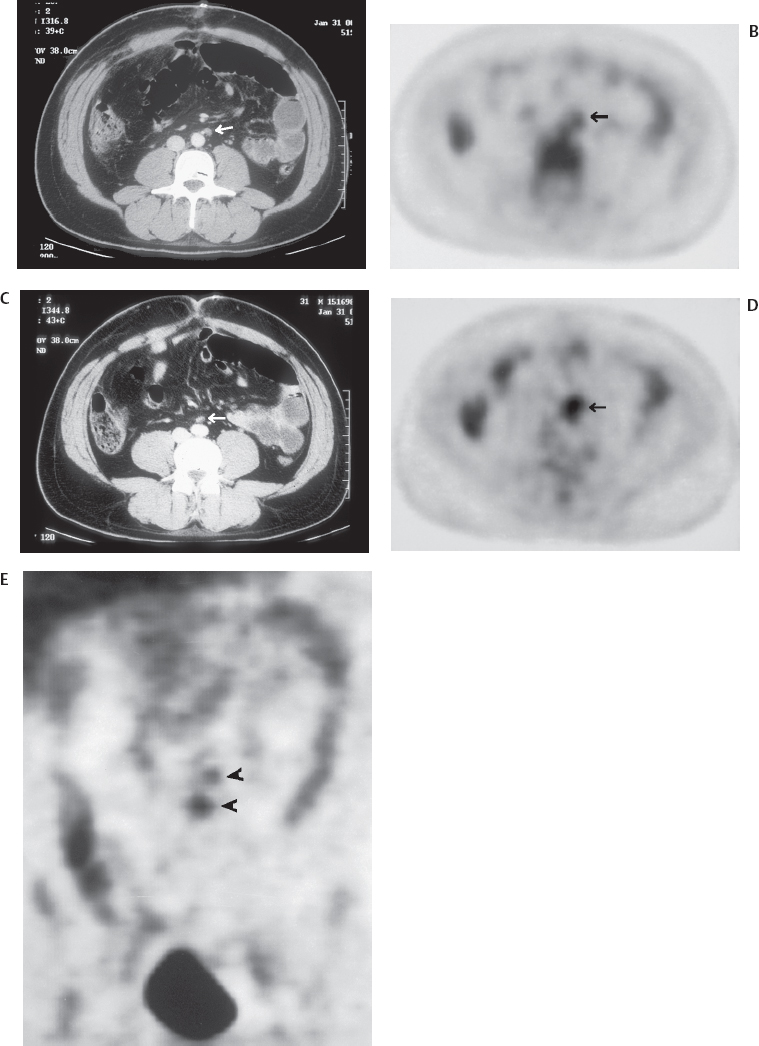
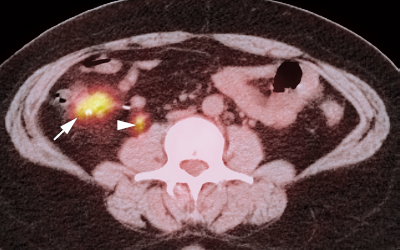
- Searching for suspected recurrent disease (rising CEA), when anatomical imaging is equivocal or negative (Figs. 24.3, 24.4, and 24.5)
- The exact utility of PET depends upon the level of CEA elevation. If CEA < 25 ng/mL, PET is helpful for triaging patients for appropriate management. If CEA > 25 ng/mL, PET is mainly helpful in confirming the presence of advanced disease and occasionally in identifying potentially resectable disease.17 A cost-effective cutoff for utilizing PET to evaluate unexplained CEA elevation may be 10 ng/mL.
- Restaging of a known recurrence if surgery is planned
- In patients screened with preoperative PET before hepatic resection, PET detects unsuspected tumor in 25% and reduces the number of unnecessary laparotomies.18 The overall 5-year survival rate after hepatic resection is 58% in colon cancer patients who have been examined with PET (compared with 30% in patients who have been assessed by conventional techniques).19
- Differentiation of posttreatment changes from recurrence
- This is a common problem in rectal cancer, as both recurrence and postradiation scars can result in abnormal soft tissue masses in the presacral space (Fig. 24.6).
- PET, hepatic. Sensitivity 80%, specificity 92%21
PET, extrahepatic. Sensitivity 91%, specificity 98%
- Lesion size. Sensitivity of PET is much lower for liver lesions < 1 cm in size.
 Primary Colonic Neoplasms
Primary Colonic Neoplasms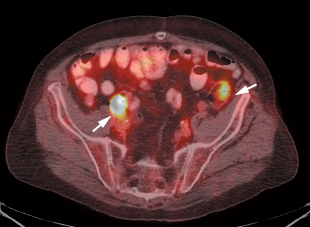
 Initial Staging
Initial Staging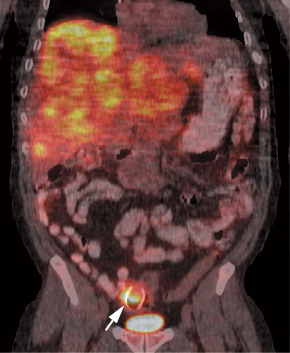
 Recurrence and Restaging15,16
Recurrence and Restaging15,16