Bilobed GB: 2 completely divided GB cavities with a common cystic duct
Duplicated GB: Duplicated GB with separate cystic ducts for each moiety
Multiseptate GB: Single GB with “honeycomb” appearance due to innumerable internal septations
Hourglass GB: Hourglass shape of GB may be congenital or acquired due to chronic inflammation
Congenital diverticulum: Usually true diverticulum that can be seen anywhere in GB
Phrygian cap: Folding of GB fundus (considered normal variant given its high prevalence)
Ectopic GB: Ectopically positioned GB has been reported in nearly every possible position in abdomen and pelvis
– Most common ectopic positions are intrahepatic, under left hepatic lobe, transverse, and retrohepatic
– Surgical removal of intrahepatic GB may be challenging
Floating or wandering GB: Mobile GB due to long mesentery, completely covered by peritoneum
– High risk of GB torsion and gangrenous inflammation
TOP DIFFERENTIAL DIAGNOSES
• Prior cholecystectomy
• Chronic cholecystitis
• Hartmann pouch of GB
• Hyperplastic cholecystoses
• Abdominal fluid collection
CLINICAL ISSUES
• Virtually always incidental finding of no clinical significance
• Floating or wandering GB has higher likelihood of torsion due to increased risk of GB “twisting” on long pedicle
(Left) Ultrasound demonstrates the characteristic appearance of a phrygian cap, with a fold near the gallbladder (GB) fundus. This is considered a normal variant given its high prevalence.
(Right) Axial T2WI FSE MR in a woman with chronic abdominal pain shows an incidental phrygian cap .
(Left) Ultrasound demonstrates many septations within the GB, creating a “honeycomb” appearance, characteristic of a multiseptate GB.
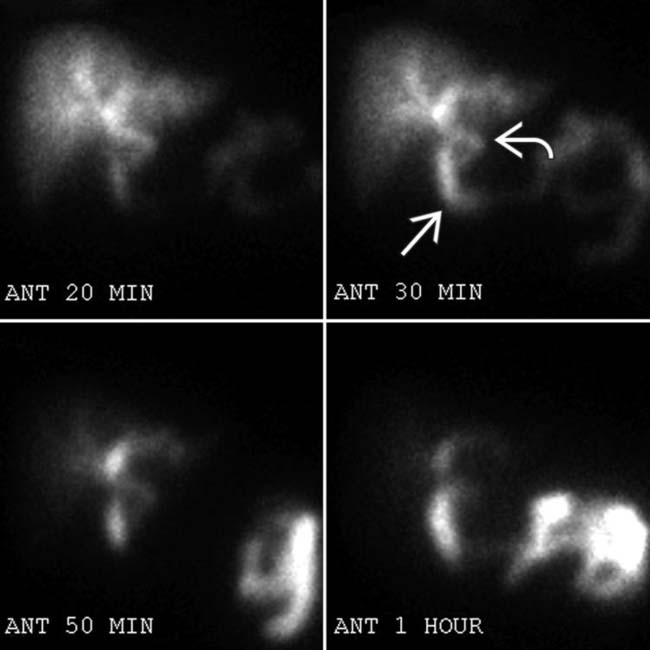
(Right) Coronal Tc-99m HIDA scan of a 54-year-old woman with abdominal pain shows progressive filling of the bile duct and proximal small bowel , but no GB activity. The patient had no operative history and multiple imaging studies confirmed GB agenesis.
TERMINOLOGY
Synonyms
• Gallbladder malformation
Definitions
• Spectrum of congenital malformations of gallbladder (GB) shape, morphology, number, or position
Agenesis of GB: Congenital absence of GB
Hypogenesis of GB: Rudimentary or atretic GB
– Differentiate from acquired microgallbladder in cystic fibrosis due to viscous bile or chronic cholecystitis
Bilobed GB: 2 completely divided GB cavities with a single common cystic duct
– Differentiate from cholecystomegaly (abnormally large GB) in sickle cell disease, pregnancy, or obesity
Duplicated GB: Duplicated GBs with separate cystic ducts for each moiety
– Cystic ducts may separately insert into extrahepatic bile duct (H-type) or have common insertion (Y-type)
Multiseptate GB: Single GB with “honeycomb” appearance due to innumerable internal septations, likely due to incomplete vacuolization of developing GB bud
Hourglass GB: Hourglass shape of GB may be due to abnormal vacuolization
– In adults, may be acquired abnormality (due to chronic inflammation and scarring)
Congenital diverticulum: Usually a true diverticulum (containing all layers of GB wall) that can be located anywhere in GB
– Differentiate from acquired diverticula due to prior cholecystitis or traction from prior surgery or duodenitis
Phrygian cap: Folding of GB fundus that is considered normal variant given its high prevalence
– Most common variant of GB shape
Ectopic GB: Ectopically positioned GB has been reported in nearly every possible position in abdomen and pelvis
– Most common positions are intrahepatic, under left hepatic lobe, transverse, retrohepatic, and retroperitoneal
Left-sided GB: Ectopic GB positioned in left side of abdomen
– Isolated or associated with situs inversus
– Cystic duct usually inserts into left hepatic duct
– May be associated with left portal vein anomalies
Intrahepatic GB: Subcapsular GB partially or completely embedded in liver
Horizontal GB: Ectopic GB within porta hepatis; usually deeply embedded in liver
Retrodisplaced GB: Retrohepatic or retroperitoneal ectopic GB
Floating or wandering GB: Mobile GB due to long mesentery, completely covered by peritoneum
– May be positioned throughout abdomen
– High risk of GB torsion and may cause pain by herniating through foramen of Winslow into lesser sac
IMAGING
General Features
• Best diagnostic clue
Abnormal shape, morphology, number, or position of GB
CT Findings
• GB agenesis: Absence of GB in patient with no history of prior cholecystectomy; should exclude prior history of cholecystectomy or ectopic position of GB before arriving at this diagnosis
Only gold members can continue reading. Log In or Register to continue







 Ectopic GB: Ectopically positioned GB has been reported in nearly every possible position in abdomen and pelvis
Ectopic GB: Ectopically positioned GB has been reported in nearly every possible position in abdomen and pelvis

 near the gallbladder (GB) fundus. This is considered a normal variant given its high prevalence.
near the gallbladder (GB) fundus. This is considered a normal variant given its high prevalence.
 .
.
 and proximal small bowel
and proximal small bowel  , but no GB activity. The patient had no operative history and multiple imaging studies confirmed GB agenesis.
, but no GB activity. The patient had no operative history and multiple imaging studies confirmed GB agenesis. Duplicated GB: Duplicated GBs with separate cystic ducts for each moiety
Duplicated GB: Duplicated GBs with separate cystic ducts for each moiety Multiseptate GB: Single GB with “honeycomb” appearance due to innumerable internal septations, likely due to incomplete vacuolization of developing GB bud
Multiseptate GB: Single GB with “honeycomb” appearance due to innumerable internal septations, likely due to incomplete vacuolization of developing GB bud Congenital diverticulum: Usually a true diverticulum (containing all layers of GB wall) that can be located anywhere in GB
Congenital diverticulum: Usually a true diverticulum (containing all layers of GB wall) that can be located anywhere in GB Ectopic GB: Ectopically positioned GB has been reported in nearly every possible position in abdomen and pelvis
Ectopic GB: Ectopically positioned GB has been reported in nearly every possible position in abdomen and pelvis















