CHAPTER 8 Cranial Meninges
The term cranial meninges refers to the three tissue layers that ensheathe the brain deep to the skull. From superficial to deep, these are the dura mater, the arachnoid mater, and pia mater.
The dura mater is also termed the pachymeninx (thick meninx). The arachnoid and pia mater, together, are the leptomeninges (thin meninges).1,2
EMBRYOLOGY
The cranial dura is mesodermal in origin, derived from the sclerotomes. The leptomeninges are ectodermal in origin, derived from the neural crest.1 The meninges form in three stages.2,3
Stage 1
From 22 to 40 days’ gestation, migrating mesenchymal cells surround the neural tube to form a reticulum between the developing nervous system and the superficial ectoderm. A vascular tunic containing immature hematogenous elements forms within this mesenchymal layer, close to the developing neural tissue.3 No distinct meninges are yet present.
Stage 2
The superficial portion of the reticulum condenses into a compact lamina that is three to four cells thick. Loosely organized mesenchyme remains deep to this lamina, between the lamina and the deeper vascular tunic. This mesenchyme is poorly cellular and has copious extracellular ground substance (glycosaminoglycans). From superficial to deep, the tissue layers are surface epithelium, compact cell lamina, poorly cellular loose mesenchyme, vascular tunic, and neuroepithelium.3 With further development, the compact cellular layer will form the outer arachnoid membrane, the dura mater, and the skull. The poorly cellular loose layer will form the subarachnoid space. Primitive pia-arachnoid cells first begin to be seen at stage 2.3
Stage 3
There is growth of the meninges and increased tissue between blood vessels.3 The compact cellular layer differentiates further into a deeper portion that will become the outer arachnoid layer and a more superficial portion that will become the dura mater. The outermost layer of the arachnoid (arachnoid barrier cell layer) is directly continuous with the innermost layer of the dura (dural border cell layer) throughout all further development. No true subdural space can be identified between the dura mater and the arachnoid.3 There is no preexisting subdural space comparable to the pleural or peritoneal cavities.4 In this stage, cerebrospinal fluid issues out from the ventricles into the poorly cellular loose mesenchyme, washes away the original extracellular ground substance, and replaces it with fluid, now designated cerebrospinal fluid (CSF). This process creates the “new” substantial, fluid-filled “layer” designated the subarachnoid space. That is, the subarachnoid space is really just a hugely expanded extracellular space. The primitive pia-arachnoid interface is organized in a simple laminar layer; in some areas, a single cell contributes different processes to both the pial surface and the inner portion of the arachnoid. Even in mature meninges, the distinction between these two layers remains difficult.3 The pial cover of the cerebral surface is incomplete in many areas. At these sites, the basal lamina of the glia limitans comes into direct contact with the subarachnoid space.3
INTERNAL ORGANIZATION/LAYERS OF AREA
Dura Mater
The cranial dura forms the thick protective layer over the brain (Fig. 8-1). It is formed of an outer endosteal layer and an inner meningeal layer.1 The outer endosteal layer is composed of elongated fibroblasts and osteoblasts. Large amounts of extracellular collagen give it strength.1 This layer attaches directly to the inner table of the skull, forming the inner periosteum of the calvaria. With advancing age, this endosteal layer becomes progressively more adherent to the skull, may calcify, and may ossify into the inner table.5
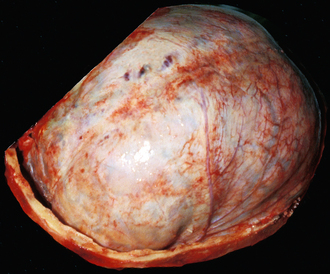
FIGURE 8-1 Anterolateral aspect of the convexity dura seen in situ after removal of the calvaria. Fresh gross anatomic specimen.
The meningeal and endosteal layers of dura remain tightly fused over most of their surface but separate from each other at two major sites. Within the skull, the inner meningeal layer of each side delaminates from the endosteal dura, reflects inward, and merges with its mate to form the double-layered dural partitions, which include the falx cerebri (Fig. 8-2), the tentorium cerebelli, and the falx cerebelli. The dural venous sinuses form where the meningeal layers delaminate from the endosteal layer of dura (e.g., superior sagittal and transverse sinuses) and in spaces left between the two meningeal layers (e.g., inferior sagittal sinus, straight sinus). At the foramen magnum, the inner meningeal layer delaminates from the endosteal dura to form the thecal sac of the spinal canal while the outer endosteal layer remains with the bone to form the periosteum of the spinal column. The fat and vascular structures of the spinal epidural space lie between the inner meningeal layer (now thecal sac) and the outer endosteal layer of dura.
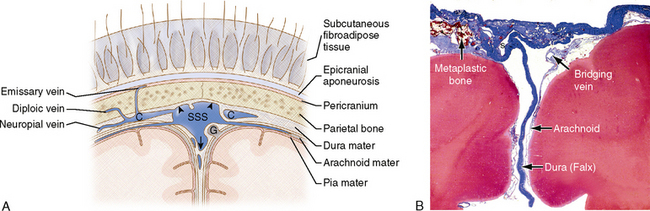
FIGURE 8-2 A, Diagram of the separation of the endosteal dura (arrowheads) from the meningeal dura (arrow). The two layers of meningeal dura fold inward to establish the falx and enclose the superior sagittal sinus (SSS). The cerebral (neuropial) veins drain into the convexity dura lateral to the sinus and travel within intradural channels (C) to enter the lateral angles of the sinus. Specialized diverticula of the arachnoid designated arachnoid granulations (G) protrude into the SSS to help reabsorb cerebrospinal fluid into the general circulation. (See also Fig. 8-6.) B, Histologic specimen. Trichrome stain shows dura as bright blue, arachnoid and associated vessels as light blue and red, and the brain as deeper red (original magnification, ×100). The superior sagittal sinus (s) is partially collapsed. Metaplastic bone is seen formed along the inner aspect of the high convexity dura. The thin arachnoid and a bridging vein lie deep to the dura.
Falx Cerebri
The falx cerebri is a broad, “sickle-shaped” double fold of meningeal dura mater that reflects downward into the interhemispheric fissure (Fig. 8-3). The outer edge of the falx attaches to the inner table of the calvaria at or near the midline. Anteriorly, it adheres to the internal frontal crest and the crista galli. Posteriorly, it adheres to the internal occipital crest and the internal occipital protuberance.6 The deep, inner edge of the falx presents a free inferior margin anteriorly but attaches strongly to the upper surface of the tentorium in the midline posteriorly. The anteriormost point at which the falx attaches to the tentorium lies at the apex of the incisura (see later) and is designated the confluence of the falx and tentorium. The superior sagittal sinus lies within the outer, attached margin of the falx superficially. The inferior sagittal sinus lies in the inner, free margin of the falx anteriorly. The straight sinus lies within the inferior margin of the falx along its attachment to the tentorium (see Fig. 8-3).7
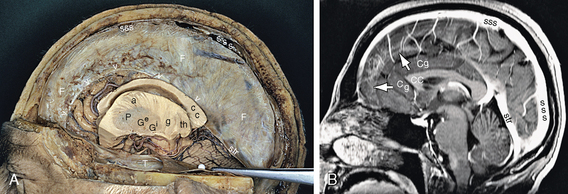
FIGURE 8-3 Falx cerebri and falcine incisura. Anterior is to the reader’s left. A, Formalin-fixed gross anatomic specimen in situ, viewed from the side after removal of much of the ipsilateral cerebral hemisphere. B, Contrast-enhanced T1W midsagittal MR image. The outer margin of the falx (F) attaches to the inner table of the skull along the superior sagittal sinus (sss) and to the tentorium along the straight sinus (str). The free margin of the falx (open white arrowheads and white arrows) descends into the interhemispheric fissure less deeply anteriorly and more deeply, posteriorly leaving a falcine incisura that is more widely open anteriorly and narrow posteriorly. The anterior cingulate gyrus (Cg), adjacent medial surface of the frontal lobe, and a large portion of the pericallosal artery lie just to each side of the falcine incisura. Further posteriorly, the free margin of the falx approximates the upper surface of the corpus callosum and the branches of the pericallosal artery pass superior to the free margin of the falx. As a consequence, midline shift is associated with greater displacement of the anterior than posterior cerebrum. In severe cases, compression (“pinching”) of the pericallosal arteries against the free margin may lead to distal pericallosal infarctions. The veins of the medial surface of the brain drain upward into the superior sagittal sinus. In A, note the relationships among the corpus callosum (cc), the anterior limb (a) and genu (g) of the internal capsule, the putamen (P), external (e) and internal (i) nuclei of the globus pallidus (g), and the thalamus (th). T, remnant of the ipsilateral tentorial leaf.
(Specimen courtesy of Drs. B. Moriggl, Munich, and T. A. Yousry, London.)
The falx develops first as two anterior and posterior portions that become a single continuous structure later.7 The anterior falx is typically shorter and thinner than the posterior portion (see Fig. 8-3) and may be perforated or even dehiscent when the posterior portion is robust (Figs. 8-4 and 8-5).7 Rarely, the anterior falx may be completely absent.7 The height of the falx varies from 28 to 48 mm anteriorly, from 41 to 62 mm in the middle, and from 40 to 62 mm posteriorly.8 As a consequence, the opening beneath the falx (incisura of the falx) is far larger anteriorly and smaller posteriorly, permitting ready shift from side to side anteriorly but limited shift posteriorly.
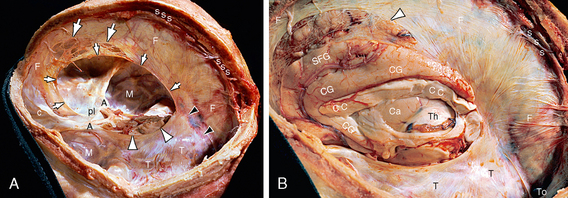
FIGURE 8-4 Falx cerebri and falcine incisura. Fresh gross anatomic specimen in situ (same specimen as in Fig. 8-9). A, View from above and the side after removal of all the supratentorial brain tissue by section through the plane of the tentorial incisura. A midline “bucket handle” of bone remains to anchor the falx to the skull. Anteriorly, the sickle-shaped falx cerebri (F) attaches to the calvaria along the internal frontal crest and descends from there to insert onto the crista galli (c) and the floor of the anterior fossa in the midline. Posteriorly, the falx attaches to the superior midline segment of the tentorium (T), enclosing the straight sinus (black arrowheads). The superior sagittal sinus (sss) courses posteriorly along the periphery of the falx. The falx is thin, shallow, and widely fenestrated (large white arrows) anteriorly leaving a wide falcine incisura (ring of small white arrows). The anterolateral edge of the tentorium (T) attaches to the superior ridge of the petrous pyramid. The free medial border (white arrowheads) of the tentorium defines the tentorial incisura. The structures within the tentorial incisura are shown in Figure 8-9. A, anterior clinoid processes; M, middle cranial fossa on each side; pl, planum sphenoidale. B, Earlier stage in the same dissection and with external compression applied to the right hemisphere. Opening the cranium and resecting the ipsilateral cerebral hemisphere exposes the falx (F), the tentorium (T), and the superior sagittal sinus (sss) that drains posteriorly into the torcular Herophili (To). The medial surface of the contralateral hemisphere is seen through the incisura of the falx, including the corpus callosum (CC), cingulate gyrus (CG), and inferior portion of the superior frontal gyrus (SFG). Marked thinning and fenestration of the anterior falx (white arrowhead) exposes more of the medial surface than is usually observed (see Fig. 8-3). Because the vertical section through the brain entered the contralateral lateral ventricle, the head of the caudate nucleus (Ca), thalamus (Th), and choroid plexus of the opposite hemisphere are also visible. The strength of the falx and the variable relationship of its free inferior margin to the cingulate gyrus and corpus callosum determine how easily the brain may shift side to side and the point at which that shift will compress the pericallosal arteries to produce distal anterior cerebral artery infarction.
(Courtesy of John Deck, MD.)
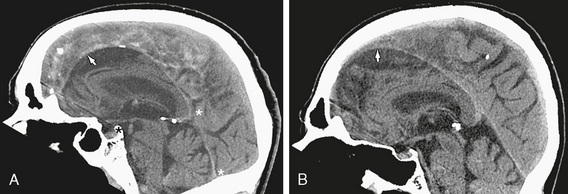
FIGURE 8-5 Falx and falcine incisura. Midsagittal reformatted CT scans with faint residual contrast hours after unrelated thoracoabdominal studies in two patients. The size, position, and configuration of the falx and falcine incisura (white arrows) are displayed in relation to the structures of the medial surface of the cerebral hemispheres. A, The falx is typical in configuration. B, The anterior falx is markedly hypoplastic creating a very large falcine incisura. Coronal images (not shown) confirmed the near absence of the anterior falx. The tentorial index is measured as the length of the closed tentorium along the straight sinus (between the two white asterisks) divided by the length of the open tentorium from the dorsum sellae (black asterisk) to the confluence of the falx and tentorium (upper white asterisk).
The falx is partially calcified in 7% of normal adult skull radiographs and partially ossified in 11% of cases.9–11 Complete ossification of the human falx is exceptionally rare.10 The calcification and ossification typically appear at the periphery of the falx in relation to the superior sagittal sinus (Fig. 8-6) and/or as islands of bone on the lateral surface of the anterior falx.9,10 These islands may contain bone marrow. Small fat deposits are found within the falx cerebri in 7.3% of cases.12
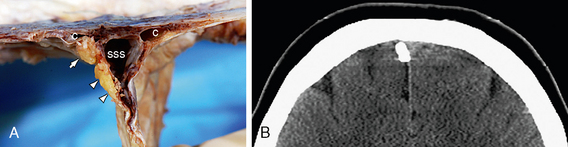
FIGURE 8-6 Ossification of the lateral wall of the superior sagittal sinus (SSS). Coronal sections. A, Gross formalin-fixed specimen. The superior sagittal sinus is thrombosed in this specimen. B, Noncontrast reformatted CT scan of a different patient. The dural walls of the SSS commonly ossify at the angle between the convexity and the sinus (arrow) and along the side wall (arrowheads). The cerebral veins do not drain directly into the side or inferior angle of the sinus. Rather, they first drain into the dura lateral to the SSS and course within the dura to enter the sinus through channels (C) leading to the lateral angles of the sinus. (See also Fig. 8-2.)
(A, Courtesy of John Deck, MD.)
Falx Cerebelli
The falx cerebelli is a midline, sickle-shaped fold of the occipital dura mater that descends from the internal occipital protuberance into the posterior fossa. It attaches peripherally to the posterior inferior surface of the tentorium cerebelli and the internal occipital crest (Fig. 8-7). Its free margin projects into the posterior cerebellar notch between the left and right cerebellar hemispheres.13,14 The falx cerebelli is typically 2.8 to 4.5 cm in length and 1 to 2 mm thick.14 It is commonly “duplicated,” even “triplicated,” forming multiple dural folds in 15.4% to 76% of cadaver dissections.14–16 The outer peripheral margin of the falx cerebelli encloses the occipital dural venous sinus.
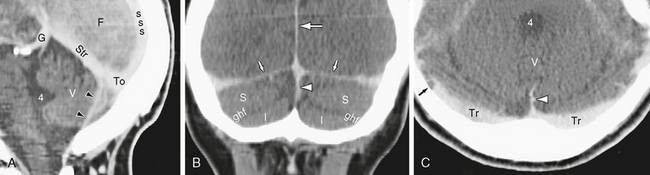
FIGURE 8-7 Falx cerebelli. Contrast-enhanced CT scan in sagittal reformatted (A), coronal reformatted (B), and axial (C) planes. The falx cerebelli (arrowheads) attaches along the inferior margin of the torcular (To) and straight sinus (Str) above and along the internal occipital crest behind to project anteriorly into the posterior cerebellar notch. It lies inferior to the tentorium (small arrows), between the two cerebellar hemispheres, and posterior to the vermis (V). It aligns only imperfectly with the falx cerebri (F, white arrow) above. In C, the lateral aspect of the right transverse sinus (Tr) shows a filling defect (small black arrow) representing a pacchionian granulation. The superior semilunar lobule (S) is separated from the inferior semilunar lobule (I) by the great horizontal fissure (ghf). 4, fourth ventricle; G, vein of Galen; sss, superior sagittal sinus.
Tentorium Cerebelli
The tentorium cerebelli (“tent”) is a taut extension of the dura mater interposed between the cerebral hemispheres above and the cerebellar hemispheres below (Fig. 8-8). The tentorium is present only in mammals and birds. It is absent in fish, amphibians, and reptiles. Like the falx cerebri, the tentorium may be partially calcified or ossified.17,18 In cats, and some other animals, the tentorium is completely ossified.17

FIGURE 8-8 Tentorium, incisura, and related dural venous sinuses. Fresh cadaver specimen seen from above after removing the cerebrum by section through the midbrain. The posterolateral borders of the two tentorial leaves (T) attach to the occipital bone along the transverse sinuses (Tr) and to the petrous ridges along the superior petrosal sinuses (Spr). The deoxygenated blood within the venous sinuses appears intensely blue. The free margins of the tentorium form a gothic arch that sweeps forward from its apex at the confluence of the falx and tentorium to insert into the anterior clinoid processes (A) bilaterally. The hiatus between the free margins is the tentorial incisura. It contains the culmen (C) of the vermis posteriorly, the midbrain (mid) and perimesencephalic cistern in the midportion, and the prepontine-suprasellar cistern anteriorly. The intracranial segments of the optic nerves (II) enter the suprasellar cistern medial to the anterior clinoid processes (A) and cross to form the optic chiasm (obscured here by residual hypothalamic tissue). Also seen are the cut anterior end of the straight sinus (s), the dura-covered veins (V) on the floor of the middle cranial fossae, the lesser wings of the sphenoid bone (sph), the planum sphenoidale (planum), and the sigmoid sinuses (Si).
Peripherally, the tentorium attaches to the rigid bony walls of the skull and encloses specific venous sinuses. The posterolateral margins of the tentorium attach to the transverse occipital ridges and the internal occipital protuberance and enclose the paired transverse sinuses and the midline torcular Herophili (confluence of the sinuses).18 The anterolateral margins of the tentorium attach to the superior surfaces of the petrous pyramids along the petrous ridges and extend from there onto the posterior clinoid processes as the petroclinoid ligaments. The anterolateral margins of the tentorium enclose the superior petrosal sinuses. In the midline superiorly, the tentorium inserts into the inferior margin of the posterior falx cerebri and encloses the straight sinus. The vein of Galen typically joins the anterior end of the straight sinus at the confluence of the falx and tentorium. It then drains through the straight sinus and torcular Herophili into the transverse sinuses.18
Centrally, the free medial margins of the tentorium sweep forward and medially from the confluence of the falx and tentorium, pass just above and lateral to the petroclinoid ligaments and posterior clinoid processes, and insert onto the anterior clinoid processes. This anatomic relationship is made possible because the interanterior clinoid distance is wider (22 to 32 mm) than the interposterior clinoid distance (17 to 25 mm) in each patient,19 allowing the free margins of the tentorium to pass lateral to the posterior clinoid processes.
Tentorial Incisura
The tentorial incisura (tentorial hiatus, tentorial notch) is the gap between the two free margins of the tentorium. The incisura has the shape of a “gothic” arch, with its apex at the confluence of the falx and tentorium and its base on the anterior clinoid processes (Fig. 8-9; see also Fig. 8-8). Its anteroposterior length is 46 to 75 mm (average, 52 mm) and its transverse width is 26 to 35 mm (average, 29.6 mm).18 For comparative anatomy and human malformation, the length of the closed tentorium along the straight sinus may be compared with the length of the open tentorium along the incisura to indicate how completely the right and left leaves of the tentorium fused together in the midline. This proportion is given as a tentorial index, defined as the length of the straight sinus from the confluence of the falx and tentorium to the torcular divided by the length of the incisura from the dorsum sellae to the confluence of the falx and tentorium (see Fig. 8-5).17 By this index the tentorium is best developed in the human and the vervet monkey.17 Note, however, that the index specifically excludes the portion of the open tentorium anterior to the dorsum sellae.
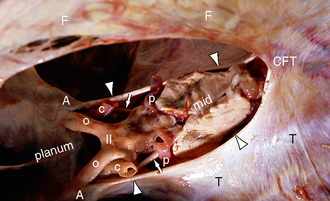
FIGURE 8-9 Tentorial incisura. Fresh gross anatomic specimen in situ, viewed from above and the side. Anterior is to the reader’s left (same specimen as Fig. 8-4). The free medial margins (arrowheads) of the tentorium (T) define the tentorial incisura. The incisura is shaped like a gothic arch with its apex at the confluence (CFT) of the falx (F) and tentorium (T) posteriorly and its base at the anterior clinoid processes (A) anteriorly. Because the width between the anterior clinoid processes is greater than the width between the posterior clinoid arteries, the free margins of the tentorium pass above and lateral to the posterior clinoid processes en route to the anterior clinoids. The anterior incisural space lies anterior to the midbrain (mid) and contains the prechiasmal intracranial optic nerves (o), the optic chiasm (II), the supraclinoid segments of the internal carotid arteries (c), the proximal posterior cerebral arteries (p), and the oculomotor nerves (small white arrows). The middle incisural space lies to each side of the midbrain. The posterior incisural space lies behind the midbrain.
(Courtesy of John Deck, MD.)
The tentorial incisura provides the only path for CSF and brain structures to pass from the supratentorial to the infratentorial compartments in either direction (Fig. 8-10; see also Fig. 8-9). When viewed from above (after removal of the cerebrum), the incisura contains the sella turcica, the brain stem, the culmen of the vermis, and the related subarachnoid cisterns. When viewed from below (after removal of the cerebellum), the incisura contains the unci of the temporal lobes, the parahippocampal gyri, the brain stem, and the related subarachnoid cisterns.18 The plane of the tentorium typically crosses the midbrain at the level of the transverse intercollicular groove between the superior colliculi above and the inferior colliculi below.
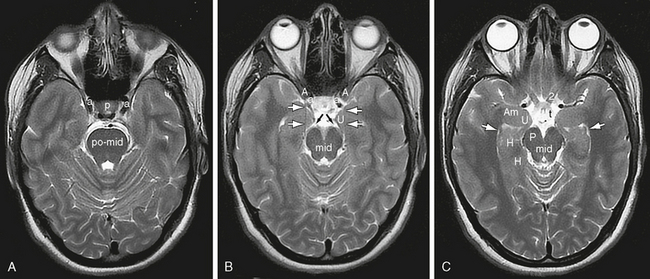
FIGURE 8-10 Tentorial incisura and the incisural CSF spaces. Axial 3T T2W MR images displayed from caudal (A) to cranial (C). A, Just inferior to the plane of the incisura, the MR image displays the junction of the pons with the midbrain (po-mid), the sella turcica containing the pituitary gland (p), and the cavernous sinuses containing the cavernous segments of the internal carotid arteries (a). B, In the plane of the incisura, the free margins of the tentorium (black lines indicated by white arrows) insert onto the anterior clinoid processes (A). The posterior clinoid processes, seen faintly, clearly lie medial to the free margins. The oculomotor nerves (CN III) (black arrows) arise from the interpeduncular fossa of the midbrain (mid) and pass forward to run in the lateral walls of the cavernous sinus. The internal carotid arteries ascend immediately medial to the anterior clinoid processes to become the supraclinoid segments of the internal carotid arteries in the next-higher section. C, Just superior to the incisura, the optic nerves (2) decussate within the suprasellar cistern, giving rise to the optic tracts (t). The amygdala (Am) forms the anteriormost wall of the temporal horn (white arrows) of the lateral ventricle. The uncus (U) forms the lateral wall of the suprasellar cistern anterior to the temporal horn. The hippocampal formation (H) forms the inferior medial wall of the temporal horn and the medial surface of the temporal lobe. The perimesencephalic cistern surrounds the midbrain. It is often divided into a crural cistern situated between the uncus and the cerebral peduncle (P) and an ambient cistern situated between the hippocampal formation and the posterolateral surface of the midbrain.
The incisura is divided into anterior, middle and posterior incisural spaces in relation to the brain stem. The anterior incisural space lies anterior to the brain stem, the paired middle spaces lateral to the brain stem, and the posterior space behind the brain stem. The anterior incisural space lies anterior to the midbrain and pons. It includes the chiasmatic and interpeduncular cisterns, so it extends from the lamina terminalis above to the interpeduncular fossa below.18 The posterior portions of the olfactory tracts (CN I), the optic nerves (CN II), and the oculomotor nerves (CN III) pass through this space. It also contains the circle of Willis, the proximal anterior choroidal arteries, the proximal superior cerebellar arteries, and the thalamoperforating arteries. The basal veins of Rosenthal course through the anterior space (and subsequently the middle and posterior spaces) to empty into the vein of Galen.18
The middle incisural space lies lateral to the brain stem and is intimately related to the hippocampal formations of the medial temporal lobes. The middle space includes the ambient and crural cisterns. The trochlear nerves (CN IV) and trigeminal nerves (CN V) pass through this space.18,20–22
The posterior incisural space is located behind the midbrain and corresponds to CSF cisterns, variably designated the quadrigeminal plate cistern, the peripineal cistern, or the cistern of the vein of Galen. The trunks and branches of the posterior cerebral and superior cerebellar arteries traverse this space. In this space, the paired internal cerebral veins join the paired basal veins of Rosenthal, the pineal veins, and the superior (galenic) veins of the posterior fossa to enter the vein of Galen.18
Meckel’s Cave
Meckel’s cave is a dural pocket situated along the medial wall of the middle fossa. It contains the trigeminal ganglion (CN V), the central processes of the trigeminal ganglion that pass posteriorly to enter the pons, and a variably large pool of CSF designated the trigeminal cistern (Fig. 8-11).22 The medial wall of Meckel’s cave is dura propria. The lateral wall is the external periosteum. The opening into Meckel’s cave lies just beneath the petroclinoid ligament where the anterolateral margin of the tentorium attaches to the posterior clinoid process. Therefore, the subarachnoid space extends into Meckel’s cave from the lateral pontine cistern of the posterior fossa, even though the dural pocket itself lies within the middle fossa. The trigeminal ganglion is situated along the anteroinferolateral wall of Meckel’s cave and there gives rise to the first (ophthalmic), second (maxillary), and third (mandibular) divisions of the trigeminal nerve.
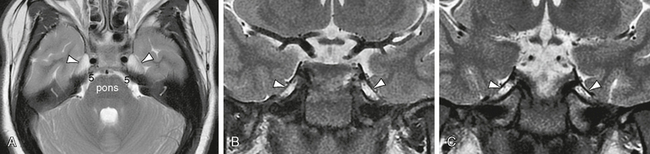
FIGURE 8-11 Meckel’s cave. Axial (A) and coronal (B, C) T2W MR images. The side walls of the sella turcica are the cavernous sinuses, containing the cavernous segments of the internal carotid arteries. Segments of cranial nerves III, IV, V1, and V2 run in the lateral wall of the cavernous sinus on each side. Meckel’s caves (white arrowheads) lie lateral to the cavernous sinuses. The medial wall of Meckel’s cave parallels the cavernous sinus. The lateral wall angles laterally, creating a triangular, CSF-filled pocket of dura situated lateral to and just slightly posterior and inferior to the cavernous sinus. The trigeminal ganglion lies along the anteroinferolateral wall of the cave. The trigeminal ganglion (CN V) gives rise to a spray of multiple thin fibers that course through the cave, join into a thick defined root (5) at the posterior aspect of the cave, and then cross the petrous apex to reach the side of the pons. The mandibular division of the trigeminal ganglion (V3) is often seen to exit the skull through the foramen ovale just inferior to Meckel’s cave.
Epidural Space
Within the cranium, there is no preexisting epidural space. An intracranial epidural space is created only when the endosteal layer of the dura detaches from the bony skull. However, meningeal arteries and veins normally course between the dura and the calvaria, forming grooves in the inner table of the skull (Fig. 8-12).1
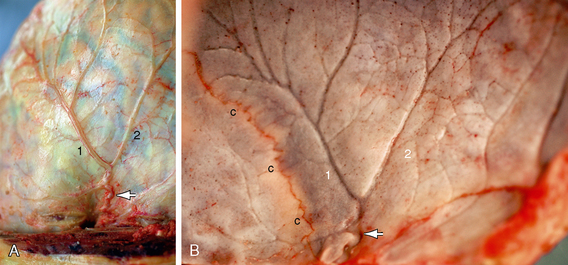
FIGURE 8-12 Epidural plane. Fresh gross postmortem specimen. A, Outer surface of the convexity dura. B, Inner surface of the apposing calvaria. The slight yellow cast is due to the patient’s jaundice. The endosteal dura adheres to the bone, leaving no normal epidural space. The middle meningeal artery (white arrow) enters the skull base at the foramen spinosum, travels laterally across the middle fossa within the epidural plane, and ascends over the convexity on the outer surface of the dura just posterior to the coronal suture (c). This artery shows modest tortuosity over a short segment inferiorly and then divides into two straighter frontal (1) and parietal (2) branches. The middle meningeal veins parallel the artery. The middle meningeal grooves in the inner table of the calvaria mirror the vessel course.
Subdural Space
There is no preexisting normal subdural space, potential or otherwise (Figs. 8-13 and 8-14).4,23–28 Studies of human cranial meninges fixed in situ show that the outermost layer of the arachnoid (arachnoid barrier cell layer) is directly continuous with, and fused to, the innermost layer of the dura (dural border cell layer).29 The dural border cell layer itself is characterized by an absence of collagen, by few intercellular connections, and by large extracellular spaces. The cells adhere very poorly to each other. Indeed, the cells of the dural border layer are more closely attached to the arachnoid barrier cell layer than to each other (see Fig. 8-14).23 This anatomic arrangement provides little cellular cohesion.29 When observed, the so-called subdural space actually results from tissue damage/trauma that shears along the dural border cell layer, creating a cleavage plane within the deepest layer of the dura.26,28 Histologic study of “subdural” collections created in guinea pigs, with special care taken to remove the meninges intact, confirmed that there were no obvious fluid-filled spaces or gaps between the dura and the arachnoid.27
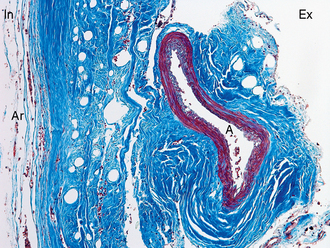
FIGURE 8-13 Histology of dura (trichrome stain, original magnification, ×100). From its external (Ex) to its internal (In) surfaces, the densely collagenous dura (intense blue stain) shows multiple parallel layers. The middle meningeal artery (A) lies at the external surface of the dura. Its adventitia is continuous with the outer layer of the dura. The loose arachnoid mater (Ar) is continuous with the internal aspect of the dura.
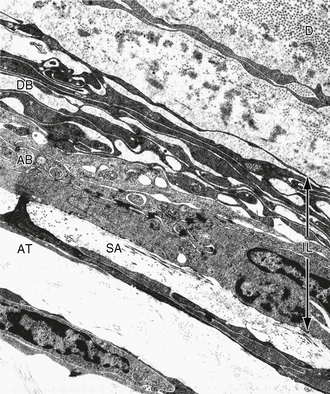
FIGURE 8-14 Undisturbed arachnoid-dural interface (fine structure, ×12,400). The interface layer (IL) lies between the subarachnoid space (SA) with its arachnoid trabeculae (AT) and the dura (D). This layer contains the arachnoid barrier (AB) cell layer and the dural border (DB) cell layer. The AB cell layer shows profuse junctional complexes with little extracellular space. The DB cell layer shows few junctional complexes. It lacks collagen and manifests multiple large empty extracellular cisterns.
(From Friede RL: Developmental Neuropathology, 2nd ed. Berlin, Springer-Verlag, 1989.)
Arachnoid Mater
The cranial arachnoid mater is a very thin membrane situated between the dura mater and the pia mater. It ensheathes the brain and continues along the cranial nerves to their point of exit from the skull.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


