• Overall prognosis for CF has dramatically improved, with average life expectancy now 35-40 years
• Respiratory failure most common cause of mortality, with liver disease 2nd leading cause of death
• Pancreatic insufficiency most common (∼ 85%) GI manifestation of CF
(Left) Axial CECT shows the classic lipomatous replacement and pseudohypertrophy of the pancreas in a young adult patient with cystic fibrosis (CF).
(Right) Axial CECT in the same patient shows dilated proximal small bowel and collapsed distal small bowel . Just proximal to the point of transition is the classic “small bowel feces sign” associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
(Left) Axial CECT demonstrates heterogeneous lipomatous replacement of the pancreatic parenchyma but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.
(Right) Coronal CECT demonstrates simple-appearing cysts in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
TERMINOLOGY
Abbreviations
• Cystic fibrosis (CF)
Synonyms
• Mucoviscidosis
Definitions
• Recessively inherited disorder of epithelial chloride transport caused by mutation of CF transmembrane conductance regulator (CFTR) gene
Pulmonary manifestations are primary cause of morbidity and mortality
CF increasingly seen to affect GI tract due to improved life expectancy
IMAGING
General Features
• Best diagnostic clue
Diffuse fatty replacement of pancreas is most common abdominal imaging finding
• Location
Most common sites of involvement are lungs, pancreas, bowel, liver, and exocrine glands
CT Findings
• Pancreatic manifestations
Early childhood: Heterogeneous attenuation of pancreas
Later childhood: Complete fatty replacement of parenchyma (often by teenage years)
Pancreatic cysts: Usually simple in appearance
– Related to inspissated secretions which lead to ductal obstruction
– Cysts are usually small (< 3 mm), but can be larger
– Cysts may diffusely replace pancreas (cystosis)
– Usually occur in patients in their 20s, and may be symptomatic as result of cyst hemorrhage
Repeated episodes of acute pancreatitis with development of chronic pancreatitis
– Pancreatic ductal strictures, dilatation, beading, etc.
May have scattered calcifications (< 10% of patients)
Increased risk of pancreatic cancer (very rare)
MR Findings
• Enlarged pancreas with diffuse fatty infiltration appears hyperintense on T1WI
• Pancreas can also appear abnormally hypointense on T1WI due to chronic pancreatitis and fibrosis
• Pancreatic cysts well demonstrated on T2WI and MRCP (hyperintense)
• Pancreatic duct abnormalities also occasionally seen
Ultrasonographic Findings
• Pancreas may be barely identifiable as result of diffuse fibrofatty replacement
• Macroscopic multiple cysts
• Hypoechoic enlargement of pancreas noted in some children with acute pancreatitis
Other Abdominal Findings
• Liver
30-50% develop hepatic steatosis ± hepatomegaly
– Can be visualized with US, CT, or chemical shift MR
– Fatty liver usually asymptomatic and does not correlate with development of CF-related cirrhosis
Cirrhosis in 5-15% of all CF patients with portal hypertension in 1-8%
 Pancreatic cysts: Usually small (< 3 mm), but can be larger and can completely replace pancreas (cystosis)
Pancreatic cysts: Usually small (< 3 mm), but can be larger and can completely replace pancreas (cystosis)




 Inspissated fecal material resulting in proximal obstruction, most often in infants (meconium ileus)
Inspissated fecal material resulting in proximal obstruction, most often in infants (meconium ileus)



 in a young adult patient with cystic fibrosis (CF).
in a young adult patient with cystic fibrosis (CF).
 and collapsed distal small bowel
and collapsed distal small bowel  . Just proximal to the point of transition is the classic “small bowel feces sign”
. Just proximal to the point of transition is the classic “small bowel feces sign”  associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
 but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.
but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.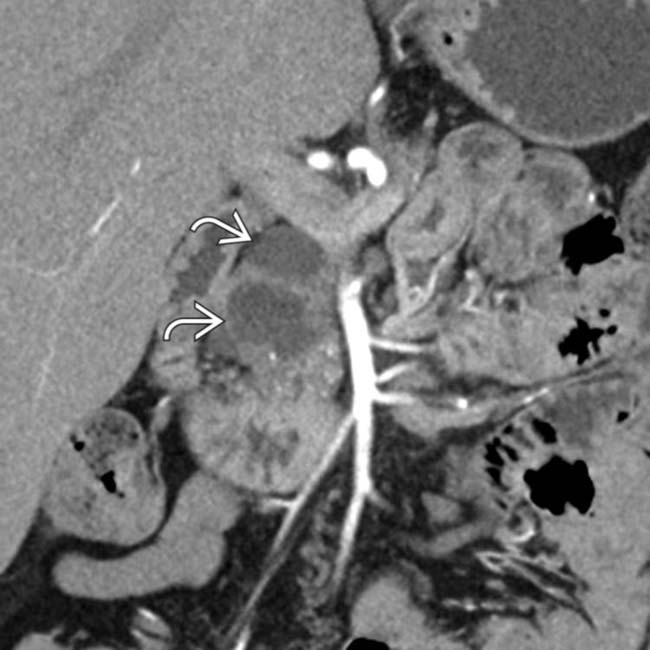
 in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.












 Gallstones in up to 1/4 of patients with CF, often with nonspecific gallbladder wall thickening and sludge
Gallstones in up to 1/4 of patients with CF, often with nonspecific gallbladder wall thickening and sludge Microgallbladder in 30% of CF patients at autopsy
Microgallbladder in 30% of CF patients at autopsy




