Narrowing of the joint space as a result of thinning of the articular cartilage
Subchondral sclerosis (eburnation) caused by reparative processes (remodeling)
Osteophyte formation (osteophytosis) as a result of reparative processes in sites not subjected to stress (so-called low-stress areas), which are usually marginal (peripheral) in distribution
Cyst or pseudocyst formation resulting from bone contusions that lead to microfractures and intrusion of synovial fluid into the altered spongy bone; in the acetabulum, these subchondral cyst-like lesions are referred to as Eggers cysts
superolateral or superomedial; medial; and axial (Fig. 13.4). The most common pattern is superolateral migration; the medial pattern is less common, whereas axial migration is only exceptionally seen. It should be kept in mind, however, that in inflammatory arthritis of the hip, such as rheumatoid arthritis, in which a previous axial migration of the femoral head is commonly associated with acetabular protrusio, degenerative changes might develop as a complication of the inflammatory process. Thus, one may see secondary osteoarthritis with axial migration (Fig. 13.5).
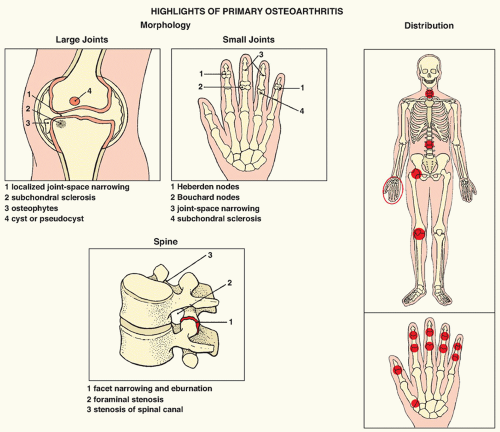 FIGURE 13.1 Highlights of the morphology and distribution of arthritic lesions in primary osteoarthritis. |
The radiographic findings are the same as those described for primary osteoarthritis, but the features of the underlying process also can often be detected. Although the standard radiographic views are usually sufficient for demonstrating these changes, CT, arthrography, or MRI may at times be needed for a more accurate assessment of the status of the articular cartilage.
TABLE 13.1 Clinical and Radiographic Hallmarks of Degenerative Joint Disease | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
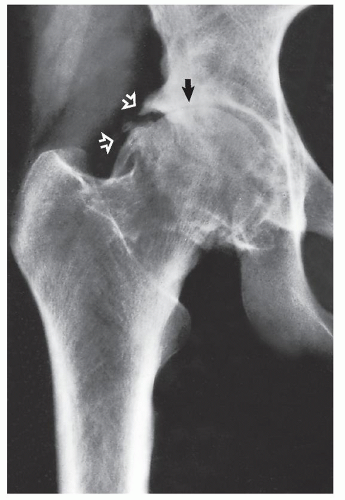 FIGURE 13.2 Osteoarthritis of the hip joint. A 51-year-old woman presented with a history of right hip pain for the past 10 years and no previous history suggesting predisposing factors for osteoarthritis. Anteroposterior radiograph of the hip demonstrates the radiographic hallmarks of osteoarthritis: narrowing of the joint space, particularly at the weight-bearing segment (arrow); formation of marginal osteophytes (open arrows); and subchondral sclerosis. Note the lack of osteoporosis. |
 FIGURE 13.3 CT of osteoarthritis of the hip. Coronal reformatted image shows diminution of the joint space, osteophytes, and subchondral cysts in the femoral head. |
 FIGURE 13.4 Migration of the femoral head. (A) Anteroposterior radiograph of the right hip of a 65-year-old woman with long-standing degenerative joint disease in both hips demonstrates superolateral migration of the femoral head, the most common pattern seen in osteoarthritis of the hip joint. Note the typical Eggers cyst in the acetabulum (arrow). (B) Medial migration of the femoral head is apparent in this 48-year-old woman with osteoarthritis of the right hip. (C) Axial migration of the femoral head is evident in this 57-year-old woman who was suspected of having inflammatory arthritis. Clinical and laboratory investigations, however, led to a diagnosis of idiopathic osteoarthritis, which was confirmed on histopathologic examination after total hip replacement. |
 FIGURE 13.5 Rheumatoid arthritis with superimposed osteoarthritis. Anteroposterior radiograph of the right hip of a 42-year-old woman with a known history of long-standing rheumatoid arthritis shows the typical changes of inflammatory arthritis, including axial migration of the femoral head and acetabular protrusio. Superimposition of secondary osteoarthritis is evident in subchondral sclerosis and marginal osteophytes. |
 FIGURE 13.6 Postel coxarthropathy. Anteroposterior radiograph of the right hip of a 72-year-old man who had pain in the hip for 4 months shows the typical appearance of Postel coxarthropathy, which often mimics Charcot joint or infectious arthritis. Note the destruction of the articular portion of the femoral head, which is laterally subluxed. The same destructive process has led to widening of the acetabulum. |
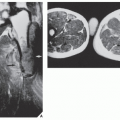
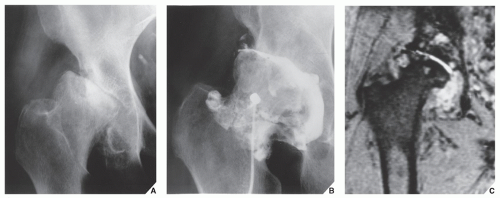 FIGURE 13.7 Postel coxarthropathy. (A) Anteroposterior radiograph of the right hip of a 44-year-old man shows destructive changes of the femoral head and acetabulum. (B) Aspiration arthrogram, which was performed to rule out infection, shows hypertrophic synovitis. (C) A gradient echo T2*-weighted MRI shows joint effusion, hypertrophied synovium, and subchondral cysts in the acetabulum and femoral head. |
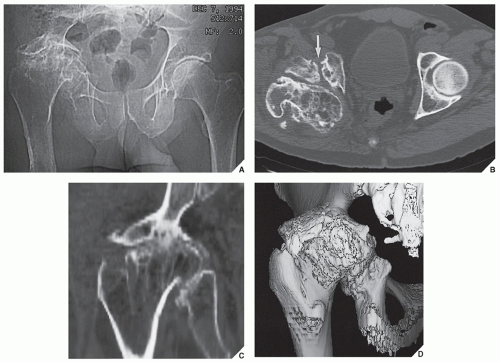 FIGURE 13.8 Posttraumatic osteoarthritis. A 64-year-old man, who in the past sustained complex right acetabular and femoral fractures, developed secondary osteoarthritis. (A) A preliminary scout CT image shows posttraumatic deformity of the acetabulum and femoral head associated with acetabular protrusio. (B) Axial CT section through both hips shows osteoarthritic changes of the right femoral head and ununited fracture of the anterior column (arrow). (C) Coronal reformatted image demonstrates significant narrowing of the joint space, deformity of the femoral head, and periarticular sclerosis. (D) 3D CT reconstructed image shows almost complete obliteration of the hip joint, acetabular protrusio, and osteophyte formation. All CT findings are consistent with posttraumatic osteoarthritis. |
on the oblique axial CT or oblique axial MR images (Fig. 13.14). Radial reformatted MR images are of particular value in this respect because they allow optimal visualization of the anterosuperior region of the femoral head/neck junction, where the most significant changes in the alpha angle occur (see Fig. 13.14B). The normal alpha angle should not exceed 50 degrees. The larger the alpha angle, the more pronounced is nonspherical shape of the femoral head, and the greater is predisposition for anterior FAI.
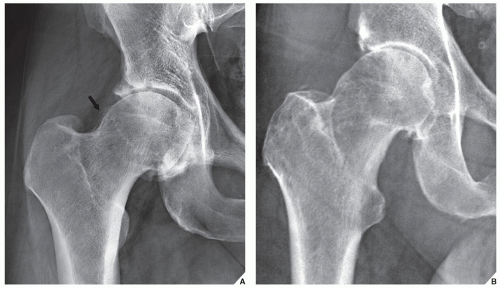 FIGURE 13.9 Cam type of FAI. (A) Anteroposterior radiograph of the right hip of a 39-year-old woman shows excessive bone buildup at the femoral head/neck junction (arrow). Note secondary osteoarthritis of the hip joint. (B) In another patient, a 41-year-old man, tubular appearance of the proximal right femur and the osseous prominence at the femoral head/neck junction assumed a “pistol grip” deformity. Also evident is osteoarthritis of the hip joint. |
 FIGURE 13.10 CT of cam type FAI. (A) Coronal reformatted CT image and (B) 3D reconstructed CT image in shaded surface display in a 34-year-old man show bone accretion at the femoral head/neck junction (arrows). |
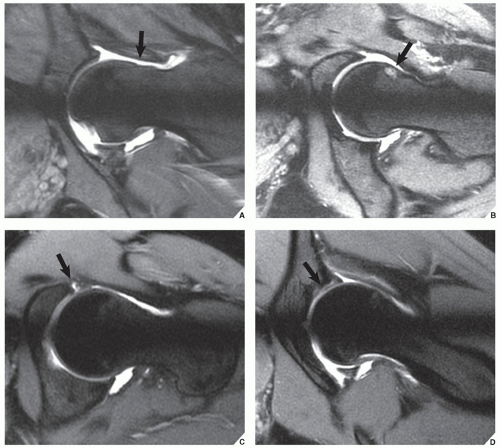 FIGURE 13.11 MR arthrography of cam type FAI. Radial reconstructed MRa images of the hip joint show various characteristic features of this abnormality. (A) In a 34-year-old woman—a decreased femoral head/neck offset associated with hypertrophic ossification (arrow). (B) In a 32-year-old woman—a fibroosseous lesion at the anterosuperior aspect of the femoral head/neck junction (arrow). (C) In a 38-year-old man—a tear of the superior anterior cartilaginous labrum (arrow). (D) In a 30-year-old woman—a delamination injury to the acetabular labrum (arrow). |
each of which may be affected by degenerative changes. The radiographic features of these changes are similar to those seen in osteoarthritis of the hip, including narrowing of the joint space (usually one or two compartments), subchondral sclerosis, osteophytosis, and subchondral cyst (or pseudocyst) formation. The standard anteroposterior and lateral projections of the knee are sufficient to demonstrate these processes (Fig. 13.15). If the medial joint compartment is affected, the knee may assume a varus configuration, which is best demonstrated on the weight-bearing anteroposterior view (Fig. 13.16A); involvement of the lateral compartment may lead to a valgus configuration (Fig. 13.16B). CT and three-dimensional (3D) reconstructed CT images may provide additional information as to the status of osteoarthritic process (Fig. 13.17). A frequent complication of osteoarthritis of the knee is the formation of osteochondral bodies, which can be demonstrated on the standard projections of the knee (Figs. 13.18 and 13.19); however, MRI may also be effective in this respect (Figs. 13.20, 13.21, 13.22). The femoropatellar joint compartment is also commonly involved in primary osteoarthritis. The lateral radiograph of the knee and axial view of the patella are the most effective means of visualizing degenerative changes of the femoropatellar compartment (Fig. 13.23).
 FIGURE 13.12 Pincer type FAI. (A) Anteroposterior radiograph of the left hip in a 29-year-old woman shows a crossover sign. Note that the posterior acetabular rim outline (yellow line) projects medially (arrow) in relation to the anterior acetabular rim (red line), indicative of acetabular retroversion. (B) In a normal hip joint, the posterior acetabular rim outline projects laterally to the posterior acetabular rim. |
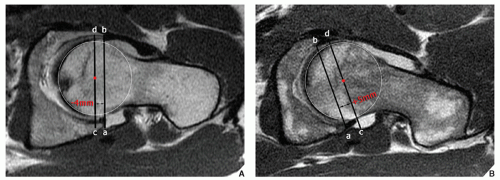 FIGURE 13.13 MRI of pincer FAI. (A) Axial oblique T1-weighted MR image shows deeply seated femoral head secondary to acetabular retroversion. Acetabular depth can be quantified by drawing a line (ab) connecting the posterior and anterior acetabular rims, and a parallel line (cd) that passes through the center of the femoral head (red dot). The distance between these two lines defines the acetabular depth, with the value being positive (+) if the center of the femoral head projects lateral to the line connecting the acetabular rims. Negative values (−) indicate deep seating of the femoral head within the acetabulum. (B) Axial oblique MR image of normal hip joint is shown for comparison. |
 FIGURE 13.14 Femoroacetabular impingement—calculation of alpha angle. The alpha angle is formed by the intersection of two lines: line AB, drawn from the center of the femoral head (A) to the point where peripheral osseous contour of the anterior femoral head intersects the extrapolated circle of the femoral head (B), and the second line AC, drawn from the center of the femoral head (A) through the longitudinal axis of the femoral neck (C). Normal alpha angle should not exceed 50 degrees. (A) Alpha angle calculated on the oblique axial CT image of the right hip in a patient with cam FAI. (B) Alpha angle calculated on the oblique axial MR image of the left hip in a patient with cam FAI. The arrows point to excessive bone formation at the anterosuperior aspect of the femoral head/neck junction. |
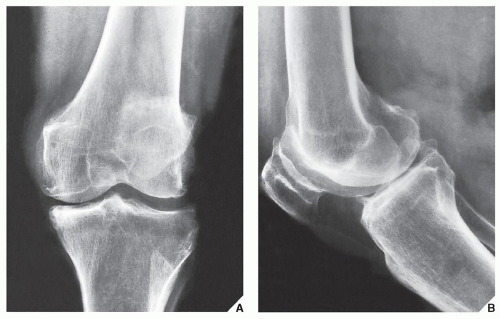 FIGURE 13.15 Osteoarthritis. Anteroposterior (A) and lateral (B) radiographs of the knee of a 57-year-old woman demonstrate narrowing of the medial femorotibial and femoropatellar compartments, subchondral sclerosis, and osteophytosis, which are the typical features of osteoarthritis. Note that osteophytes that were not obvious on the frontal projection are much better demonstrated on the lateral radiograph. |
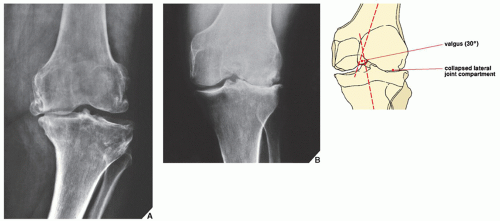 FIGURE 13.16 Osteoarthritis. (A) Weight-bearing anteroposterior radiograph of the knee of a 58-year-old woman demonstrates advanced osteoarthritis of the medial femorotibial joint compartment, which has led to a varus configuration of the joint. (B) Involvement of the lateral femorotibial joint compartment in advanced osteoarthritis as seen on this weight-bearing anteroposterior radiograph of another patient has resulted in a valgus configuration. |
 FIGURE 13.17 3D CT of osteoarthritis. (A) Radiograph of the right knee of a 58-year-old man shows advanced osteoarthritis. (B,C) 3D reconstructed CT images in shaded surface display demonstrate advanced three-compartmental osteoarthritis.
Related posts: Radiologic Evaluation of Skeletal Anomalies Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|