When involving abdominal wall, often involve rectus or oblique muscles, frequently at incision sites
When involving mesentery, may retract or compress adjacent bowel loops ± small bowel obstruction
• Usually solid with well-defined margins (but can be infiltrative in appearance)
• CT: Hyperdense to muscle on NECT and usually hypoenhancing on CECT (but rarely avidly enhancing)
• MR: Classically thought to be low signal on all MR pulse sequences due to fibrous content but this is unreliable
Usually heterogeneously high signal on T2WI and STIR
Usually homogeneously isointense/hypointense on T1WI
Bands of internal low signal on all pulse sequences
TOP DIFFERENTIAL DIAGNOSES
• Soft tissue sarcoma
• Leukemia and lymphoma
• Carcinoid tumor
• Primary small bowel tumors extending into mesentery
PATHOLOGY
• Strong associations with Gardner syndrome and familial adenomatous polyposis (FAP)
• Other major risk factors include previous abdominal surgery (75% of cases), trauma, or oral contraceptives
CLINICAL ISSUES
• Complications arise from locally aggressive growth pattern with compression and invasion of adjacent structures
• Surgical resection difficult in many cases as result of involvement of adjacent critical structures
• Recurrence after surgery is very common
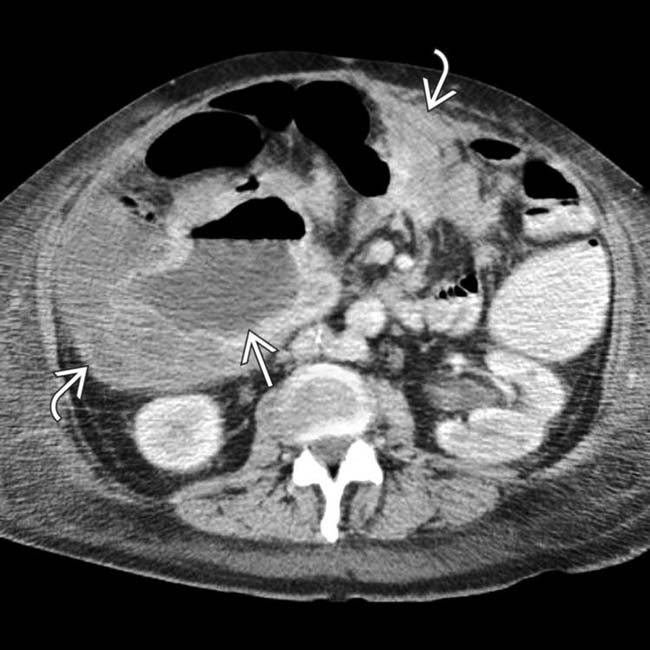
(Left) Axial CECT in a 43-year-old man with Gardner syndrome shows a huge mesenteric mass that encases and partially obstructs the small bowel. A portion of the mass has central cavitation and an air-fluid level that might be misinterpreted as aneurysmal dilation of the bowel lumen.
(Right) Gross pathology of the resected mass from the same case shows encasement of the small bowel. A portion of the mass is necrotic and communicates with the bowel lumen, accounting for the air-fluid level on CT.
(Left) Axial CECT demonstrates a relatively homogeneous, enhancing, well-circumscribed mass in the right anterior pelvis.
(Right) Axial CECT in the same patient demonstrates a very similar-appearing smaller mass in the more inferior pelvis. This was a patient with Gardner syndrome, and both of these lesions were found to represent desmoid tumors.
TERMINOLOGY
Synonyms
• Deep or aggressive fibromatosis
Definitions
• Rare, benign, locally aggressive, nonencapsulated mesenchymal neoplasms of connective or fibrous tissue
IMAGING
General Features
• Best diagnostic clue
Small bowel mesentery or abdominal wall mass arising at site of scarring from prior surgery
• Location
Can be intraabdominal or extraabdominal (including abdominal wall)
– Abdominal desmoids
Account for 2/3 of all desmoid tumors
Tumors associated with Gardner syndrome or familial adenomatous polyposis (FAP), usually intraabdominal
Most commonly occur in small bowel mesentery, but can occur nearly anywhere
– Extraabdominal
Pregnancy-related desmoid tumors tend to occur within abdominal wall
1/3 occur in shoulder and upper extremity
∼ 20% in chest wall, ∼ 10% in head and neck
Musculature most often involved: Rectus, internal/external oblique, psoas, pelvic (rare)
• Size
Mass may range from 4-20 cm
• Morphology
Well- or ill-defined, tan or white, hard fibrous mass
Clear, lobulated margin (75%)
Ill defined, infiltrative (25%)
• Key concepts
Locally aggressive primary mesenchymal tumor
– Sometimes classified as low-grade fibrosarcoma or subgroup of fibromatosis
– Tend to arise in musculoaponeurotic planes
– Tend to invade locally, recur after treatment, and grow very rapidly, especially in Gardner syndrome
– May involve bowel loops, bladder, ribs, pelvic bones, and virtually any other structure
Desmoids can be solitary or multiple (15% of cases)
Etiology
– Most cases are sporadic
– 75% of patients with desmoid tumors have had prior abdominal surgery
Periampullary, adrenal, thyroid, and liver carcinomas
18-20% of patients with Gardner syndrome develop desmoids
– Accounts for 45% of fibrous lesions in Gardner syndrome
CT Findings
• Abdominal wall desmoids
Usually solid with well-defined margins (but can be infiltrative in appearance)
Homogeneous or heterogeneous density on NECT (hyperdense compared to surrounding muscle)
Usually hypoenhancing on CECT (but rarely avidly enhancing)
Often involve rectus or oblique muscles, frequently at incision sites
• Mesenteric desmoids
Soft tissue mass with well-defined or ill-defined margins
Hyperdense relative to muscle on NECT with variable, heterogenous enhancement on CECT
Whorled appearance: Radiating fibrotic strands into adjacent mesenteric fat
May displace, retract, or compress adjacent bowel loops ± small bowel obstruction
± infiltration into adjacent organs and musculature
Calcification uncommon
MR Findings
• Can be poorly marginated or very well circumscribed
Often will cross fascial boundaries (1/3 of cases) and may be lobulated or infiltrative
• Classically thought to be low signal on all pulse sequences due to fibrous content
Not a consistent or common feature, and may be seen with other entities (including malignancies such as fibrosarcoma and malignant fibrous histiocytoma)
Usually homogeneously isointense or mildly hypointense on T1WI
Heterogeneously high signal on T2WI and STIR
– Higher T2 signal more common with actively growing or aggressive desmoids
Bands of low signal on all pulse sequences (likely corresponding to bands of fibrosis and collagen) seen in 2/3 of cases
Only gold members can continue reading. Log In or Register to continue




 that encases and partially obstructs the small bowel. A portion of the mass has central cavitation
that encases and partially obstructs the small bowel. A portion of the mass has central cavitation  and an air-fluid level that might be misinterpreted as aneurysmal dilation of the bowel lumen.
and an air-fluid level that might be misinterpreted as aneurysmal dilation of the bowel lumen.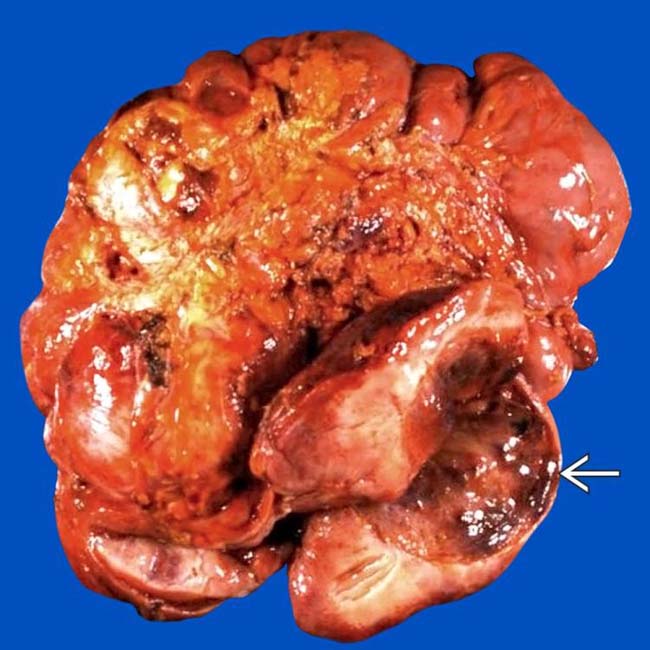
 and communicates with the bowel lumen, accounting for the air-fluid level on CT.
and communicates with the bowel lumen, accounting for the air-fluid level on CT.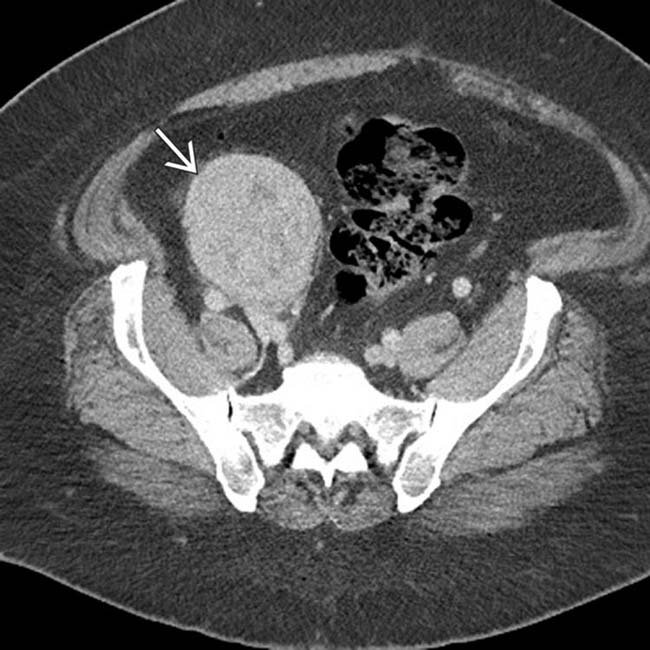
 in the right anterior pelvis.
in the right anterior pelvis.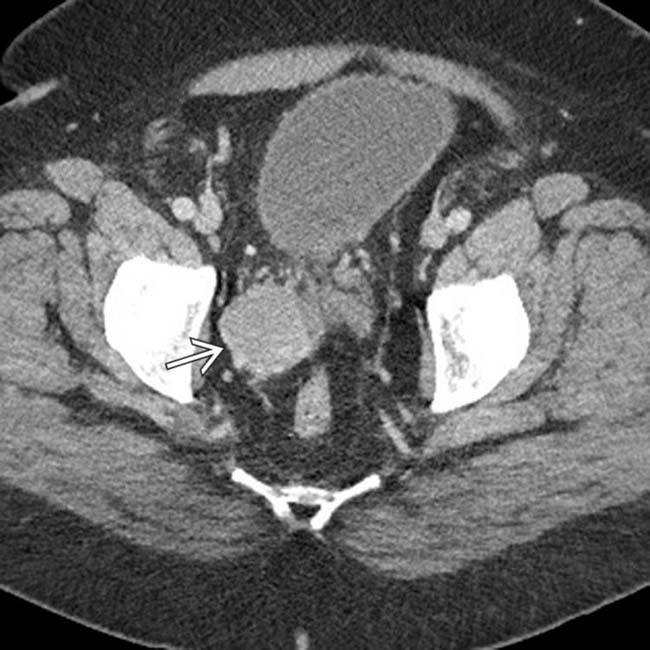
 in the more inferior pelvis. This was a patient with Gardner syndrome, and both of these lesions were found to represent desmoid tumors.
in the more inferior pelvis. This was a patient with Gardner syndrome, and both of these lesions were found to represent desmoid tumors.






























 Not a consistent or common feature, and may be seen with other entities (including malignancies such as fibrosarcoma and malignant fibrous histiocytoma)
Not a consistent or common feature, and may be seen with other entities (including malignancies such as fibrosarcoma and malignant fibrous histiocytoma) Bands of low signal on all pulse sequences (likely corresponding to bands of fibrosis and collagen) seen in 2/3 of cases
Bands of low signal on all pulse sequences (likely corresponding to bands of fibrosis and collagen) seen in 2/3 of cases







