Figure 22.1.1
Ultrasound-guided amniocentesis. Ultrasound has been used to guide a needle (arrowheads) into the amniotic fluid.
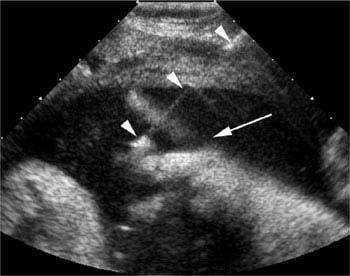
Figure 22.1.2
Continuous sonographic monitoring of fetal movement during amniocentesis. A fetal hand (arrow) is in proximity to the needle (arrowheads) during amniocentesis.
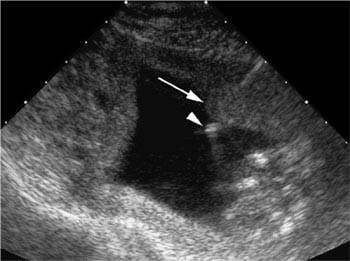
Figure 22.1.3
Continuous sonographic monitoring detecting uterine contraction during amniocentesis. A uterine contraction (arrow) comes close to enveloping the needle tip (arrowheads) during amniocentesis. If the contraction increases in size, the needle will have to be advanced to remain within the amniotic fluid.
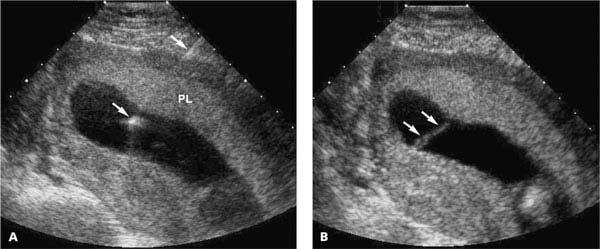
Figure 22.1.4
Ultrasound-guided amniocentesis through an anterior placenta. A: The amniocentesis needle (arrows) traverses an anterior placenta (PL). B: After the needle was removed, streaming of blood (arrows) is seen into the amniotic cavity from the puncture site in the placenta. The bleeding stopped after approximately 30 seconds.
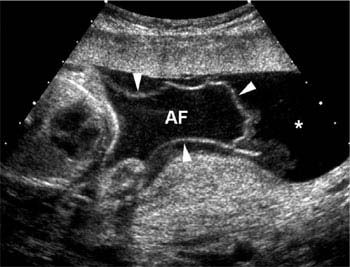
Figure 22.1.5
Chorioamniotic separation following amniocentesis. The amnion (arrowheads) is separated from the chorion on this 22-week scan, with amniotic fluid (AF) inside the amniotic sac and leaked fluid (*) between the amnion and chorion.
22.2. Chorionic Villus Sampling
Description and Clinical Features
In the mid-first trimester, chorionic villi proliferate at the implantation site to form the chorion frondosum, which interdigitates with the maternal decidua basalis to form the placenta. Because the chorionic villi develop from the fertilized egg, these cells have the same genetic makeup as the fetus. Sampling and testing the villi, by direct examination of the mitotically active cytotrophoblasts and culture of the mesenchymal cells, provide chromosomal and biochemical information about the fetus.
Chorionic villus sampling (CVS) is usually performed at 10–12 weeks gestation, and karyotypic results are available within 1–7 days. CVS thus yields chromosomal information earlier in the pregnancy and more quickly than amniocentesis. Potential disadvantages of CVS include the following:
Pregnancy loss: Some studies suggest a slightly higher rate of pregnancy loss after CVS than amniocentesis, though the risks are difficult to compare because CVS is performed earlier in pregnancy when background loss rates are higher.
Inaccurate karyotype: The placenta and fetus can occasionally have different karyotypes. When this happens, CVS provides incorrect information about the fetal karyotype. Contamination of the sample by maternal decidual cells is another potential source of error.
Fetal malformations: An increased incidence of limb reduction anomalies after CVS has been reported. This risk appears to be restricted to CVS performed before 10 weeks gestation.
Sonography
CVS is performed under continuous ultrasound guidance. The procedure can be performed through one of two approaches:
Transabdominal (Figure 22.2.1): The needle is inserted percutaneously through the maternal abdominal wall and directed into the placenta. Suction is applied as the sampling device is moved back and forth across the placenta.
Transcervical (Figure 22.2.2): A catheter is inserted through the cervix and directed via transabdominal ultrasound guidance into the placenta. Suction is applied as the catheter is moved back and forth across the placenta.
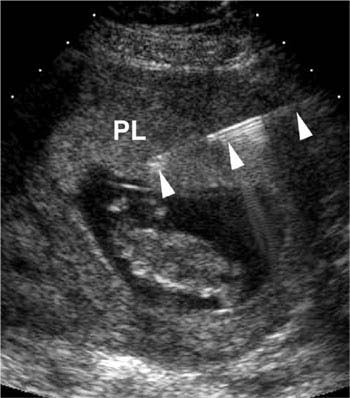
Figure 22.2.1
Transabdominal chorionic villus sampling. A needle (arrowheads), inserted percutaneously through the anterior abdominal wall of the mother, extends into the placenta (PL).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


