(1)
Department of X-Ray and MRI, RailWay Clinical Hospital, Yaroslavl, Russia
Abstract
Ureteral diverticulum (UD) is a saccular outpouching of the ureteral wall which may vary in size and location. Diverticulum wall consists of the same layers as the ureter. The inner surface of UD is covered with urothelium; the submucosal layer is usually subtle. In the embryologic aspect, UD are additional outpouchings of the caudal end of the coelenteron, and they develop as an additional ureter anlage. UD can be found in any part of the ureter, on one or both sides, but the most frequent location is the pelvic area, more often on the right.
Ureteral diverticulum (UD) is a saccular outpouching of the ureteral wall which may vary in size and location. Diverticulum wall consists of the same layers as the ureter. The inner surface of UD is covered with urothelium; the submucosal layer is usually subtle. In the embryologic aspect, UD are additional outpouchings of the caudal end of the coelenteron, and they develop as an additional ureter anlage. UD can be found in any part of the ureter, on one or both sides, but the most frequent location is the pelvic area, more often on the right.
UD, the same as diverticula of any other part of the urinary tract, are divided into congenital and acquired ones. According to some authors, UD is mostly of acquired nature and is related with ureter diminution caused by various traumas or by consequences of surgeries or resulting from ureter wall decubitus formed under a concrement and followed by an infection which weakens the ureter wall and provokes UD formation [1–3].
Congenital UD are observed very rarely and are usually discovered accidentally. Harlin and Atkinson [4] found only 18 descriptions of congenital UD in the literature and added an observation of their own. Desgrez [5], who described UD in the lower part of the right ureter in 1983, considered his observation to be the 26th case in the global literature. Sparsity of UD is also confirmed by statistics from the Mayo Clinic (1977) [6], where only 12 UD cases were discovered for 25 years (they are not divided into congenital and acquired in the report), and by statistics from the urological 100-bed clinic Perm Medical Academy (2008) [7], where for the same period, 25 years, only one patient was diagnosed with ureteral diverticulum among the 766 patients with ureteral abnormalities, while the latest publication on a congenital UD issued in 2005 is only the third one in the Japanese literature [8].
The first publication in the domestic literature devoted to demonstration of a hydronephrosis preparation containing a ureteral diverticulum (UD) was made by N. V. Sklifosovsky, an outstanding Russian surgeon [9].
From time to time, individual personal observations of UD are reported in the domestic and overseas literature which are supplemented by various statistical reference data, from singular cases to dozens of descriptions collected by various authors [3, 8, 10–40].
According to Culp [41], the specific sign of UD which is considered a rare congenital abnormality is the presence of a saccular outpouching of the ureter wall. This protrudes at an angle from the main ureter and maintains the minute structure typical for the ureter. UD length always exceeds its double diameter. The author observed three girls (4, 11, and 13 years old) with UD. No specific signs of UD were found. All the patients had the clinical presentation of chronic pyelonephritis. UD can be treated only by surgical methods. One patient had nephroureterectomy; the others had UD resection. All UD contained cloudy urine. Histologic examination revealed UD wall structure identical to the ureter structure with signs of inflammatory infiltration.
According to Delmas and Delmas [10] UD are often discovered incidentally. The author described a 77-year-old patient who had multiple UD on the left in the pelvic area, while the upstream parts of the upper urinary tract remained unchanged. These diverticula were “accidentally” discovered when the patient was examined for painless intensive macrohematuria which had developed due to overdose of blood thinners. Based on that observation and 30 more UD cases collected from the reference literature, it is considered that UD, including multiple ones, are usually discovered incidentally. In men UD were found more often (22 observations), and about half of the patients had bilateral UD (16 observations). Deranged urodynamics in the upper urinary tract was discovered in 15 patients, and 9 patients had urinary tract infections
There is a description of an incidental UD finding which was made during examination of children with recurrent urinary tract infections. 17 UD are described including 14 pediatric patients. All patients had VUR which was complicated with recurrent urinary infections in 13 patients, with various dysuric phenomena in 3 patients, with enuresis in 2 patients, and with macrohematuria in 2 patients. Thirteen patients had retentional changes on UD side. The main reason for X-ray examination was VUR, while the discovered UD were, according to the authors, an “incidental finding” [29, 30]. These authors emphasize the fact that in descriptions by other authors, VUR is mentioned as a very rare phenomenon which accompanies UD and facilitates its diagnostics.
Sparsity of UD is confirmed by observation of six patients: two patients had UD on the left and four on the right. One patient was suspected to have an ovarian cyst. Another female patient had a necessary nephrectomy due to purulent pyelonephritis which developed after diverticulectomy and ureteroneocystostomy [27].
Aivazyan A.V. and Vojno-Yasenetsky A.M. in their review of literature on UD provide data that in 1936 Brown collected 9 descriptions of congenital UD from the literature, in 1950 Harlin and Atkinson collected as many as 18 descriptions of congenital UD and added one of their own (a 56-year-old male), and in 1959 Stachler discovered 13 more observations of this kind [28].
One of the authors [15] described his observation of a 5-year-old boy with a 5.0 × 3.0 cm UD who finally had the diverticulum Resection. Six months after the surgery, function of the kidneys was unchanged. Ectasia of the ureter up to 1.5 cm along 5–6 cm of the pelvic part over the area of UD resection still remained.
UD, the same as diverticula of any other part of the urinary tract, are divided into congenital and acquired ones. Congenital ureteral diverticula are observed in extremely rare cases. In ureterograms they look like ureteral wall outpouchings, and since this congenital abnormality is usually related with irregularity of urine passage down from the upper urinary tract, it may be combined with hydronephrosis and hydroureter. Congenital UD are usually small. In the literature only a few cases of large diverticula observations are described [3]. Diverticulum may appear in any part of the ureter.
Congenital ureteral diverticulum is rather a rare abnormality of the urinary tract. In report [30] only 15 cases out of 52 were classified as congenital. In majority of patients clinical presentations appear as late as above 20 years old and are as follows: pains and urinary tract infections; in some cases, there is a palpable formation which causes various diagnostic errors.
Congenital UD results from disturbances of embryogenesis of the urogenital system. Some researchers regard congenital UD as an incomplete double ureter. That is, a blind-ended branch of the ureter formed at its incomplete duplication, a kind of ureter appendage which can spring at any level.
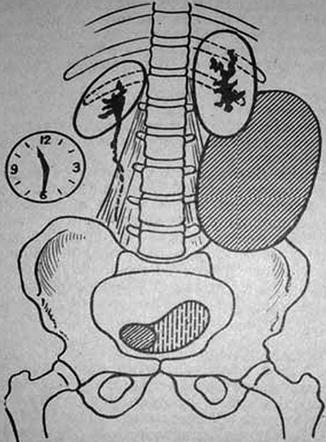
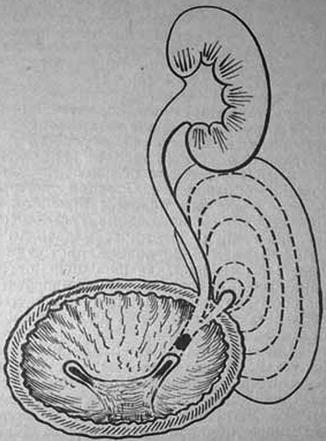
In the Russian literature [18], a 24-year-old female patient is described (13-year catamnesis) who was urgently operated on for a twisted cyst of the left ovary which was not found. One month later she was admitted to the gynecology department again and diagnosed with acute parametritis and 16-week pregnancy. The second surgery was performed in the urology department with preoperatively diagnosed hydronephrosis on the third accessory kidney on the left (which contained 1.5 l of urine). The patient was operated on by A. Ya. Pytel who carried out ureterocystoneostomy. The removed preparation contained no layers which would be typical for the ureter wall, but the author explained it by UD expansion from 1.0 cm in diameter to a gigantic stretched bag where granulation tissue with cicatrization started to prevail due to a prolonged inflammatory process (Figs. 2.1 and 2.2).
As Aivazyan and Vojno-Yasenetsky note [28], congenital ureteral diverticulum is a shallow formation which is nearly always located in the pelvic area of the ureter and is connected with its lumen by means of a more or less wide duct. UD may have various shapes (round, ovoid, saccular, irregular, tubulous, etc.). UD usually has a small capacity, from 3 to 15 ml. UD wall structure vaguely resembles the structure of the ureter wall. UD usually has urothelial lining and a muscular layer, but in most cases urothelial cells are subject to metaplasia, and often they have pseudopolypous proliferations; the structure of muscular layers is irregular, and sometimes only individual muscular fibers are found which are located among the coarse fibrous tissue.
True UD (unlike blind-ended branches of accessory ureter) are not necessarily related with duplication or divarication of the ureter. In many cases UD are multiple and bilateral. Parts of the ureter which are located above UD, as well as the pelvicalyceal system and the kidney, are developed properly; sometimes more or less prominent secondary retentional changes are present.
Aivazyan and Vojno-Yasenetsky [28] classify UD as a congenital abnormality of the 1st clinical and functional type (congenital abnormalities which do not require treatment). Complications and concomitant diseases are very rare in the case of UD. This makes the theory of their acquired nature [18] caused by congenital or acquired diseases unpersuasive. Pytel and Tchebanyuk [37] suppose that “the diverticulum develops as an accessory ureter anlage.” In the opinion of Aivazyan and Vojno-Yasenetsky [28], the most probable explanation is the following: the blind-ended accessory ureter of UD at various stages of their embryo morphogenesis is a divaricated branch of the metanephric duct which stopped to develop. In case an accessory ureter forms, the development stops later when a structure identical with the normal ureter is completed but has a blind end. In case of UD divarication is not followed by further growth; thus, a saccular formation appears which is connected with the main ureter and bears signs of histogenetic affinity to the ureter (urothelial lining, muscular layer), but its structure is not at all similar to a normal or blind-ended ureter. In the opinion of most researchers [27–30], the congenital UD is a duplex ureter which has an inlet and outlet leg or a blind-ended ureter branch. UD development may be stimulated by concurrent infections, reflux, and presence of stones. UD formation is caused by an abnormality of the ureter area where autonomic ganglions are absent, but there is a prominent rugosity of the mucosa which disturbs urodynamics.
As noted by Pytel and Pytel [38], in case two ureters are discovered on one side and one of them is blind ended, it must be kept in mind that the same presentation can be observed in case of a ureteral diverticulum (UD). According to Pytel and Pytel [38], UD is mostly of acquired nature and is related with ureter diminution caused by various traumas or by consequences of surgeries or resulting from ureter wall decubitus formed under a concrement.
The hypothesis of acquired UD nature also has it that UD develops due to overlay of infectious process and obstructed urine drainage. The infectious inflammatory process weakens the ureteral wall in some areas, and high pressure of urine provokes diverticula formation.
As mentioned above, UD is classified as a rare abnormality which consists of the formation of a saccular outpouching in the ureteral wall that may have various size and location but is mostly located on the right and in the pelvic area of the ureter. Extremely rare UD is found in the ureter area near the renal pelvis. Bilateral UD are also described. Hyperinflated UD constricts the adjacent part of the ureter, causing its obstruction with respective clinical presentations. Ureteral diverticulum has the same complications as calyx diverticulum: inflammation, lithogenesis, ureteropyelocaliectasis, and perforation.
True UD (different from blind-ended branches of accessory ureter) are not necessarily related with ureter duplication or divarication. UD are often multiple or bilateral. Parts of the ureter which are located above UD, as well as the pelvicalyceal system and the kidney, are developed properly; sometimes more or less prominent secondary retentional changes are present. Three patients are described [28] with small (up to 2–3 cm) solitary UD in the perivesical part of the ureter which had ovoid shape and were connected with the ureteral lumen by a narrow duct; no retentional changes of the UUT were present. All UD were “accidental” findings made during examinations for hematuria, enuresis, and proteinuria. No indications for surgical treatment of UD were found.
The majority of authors, as emphasized in Aivazyan and Vojno-Yasenetsky [28], also believe that diverticulectomy and resection of the perivesical part of the ureter in combination with ureterocystoneoanastomosis are justified only in rare cases, when UD has unusually big size, lithogenesis is present, or there are prominent disturbances of urodynamics on the UD side.
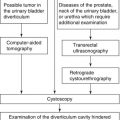
Excretory urography is the main method of UD diagnostics. Excretory urograms display a globular or saccular accessory cavern which has a sharp outline and is directly adjoining the ureter, the ureter being constricted in that area. The rate of the contrast medium accumulation in the cavity of the UD increases on delayed images, while UD opacification persists after the contrast medium discharge from the upper urinary tract.
As emphasized by [28, 38], the main method of UD diagnostics is X-ray examination. If the kidneys’ function is satisfactory, usually the boundary of the ureter and its diverticulum is clearly seen in excretory urograms all over the ureter length. The authors explain these presentations by the pendulent ureteroureteral reflux (PUR) at the point of the UD divarication. At a diminished function of the kidneys, the authors used cystography: If PUR was present, the contrast medium filled both the ureter and its diverticulum. If PUR was absent, diagnostics were made by means of retrograde ureteropyelography which permitted to define the exact location and size of the diverticulum as well as the spot of its divarication from the main ureter.
In retrograde ureterograms UD are often diagnosed as strictures since the diverticulum neck is narrowed and, therefore, it may be difficult to achieve a good diverticulum filling with the contrast medium. It is not always possible to opacify the UD cavity during retrograde urography because of its inlet narrowing or the presence of a concrement; that’s why in many cases UD are discovered only during a surgery [14, 19].
The only illustration present in the domestic literature is the one in the work by Lopatkin and Lyulko [39] which in turn was copied from a work by Desgrez [5] who described the 26th observation of UD. A 73-year-old woman was admitted for examination for recurrent cystitis. The cystitis recurred about two times a year and was relieved efficiently by short-term usage of antibiotics. Microhematuria persisted in the patient, and due to that reason, EU was performed. A specific image of the lumbar part of the left ureter was discovered which looked like a bunch of grapes. UD was described for the first time in 1957 (Holly and Sumead). Based on the analysis of the data from the literature and the abovementioned observation, it is emphasized that UD is found mostly in men aged 23–85 years old. No similar observations in children have been reported up to the moment. Twelve patients had bilateral UD, 11 patients had UD on the left, and 3 patients had UD on the right. Often patients had infections in the urinary tract. Some authors observed hindrance to urine drainage in UD patients. UD symptomatology is almost absent which is confirmed by long-term observations (up to 8–15 years) in four patients with UD. This is explained by the fact that only a few histologic observations are available and no surgeries for UD were carried out. However, two patients had the ureter with UD removed due to other diseases (1, cancer; 1, pyelonephritis). The first observation includes a moderate ureter myopachynsis, and the second observation includes a pseudogonorreha. Prosection of the first patient with UD revealed a minimal external bulging of the ureter wall (Fig. 2.3).

Fig. 2.3
Excretory urogram. Left ureter diverticulum (After Lopatkin and Lyulko [39], Fig. 131, p. 176)
The development of the secondary diverticulum in the part of the left ureter located at the renal pelvis with its congenital valves along with hydronephrosis was described by Kim et al. (2004) (Fig. 2.4).

Fig. 2.4
Retrograde ureteropyelogram in case of congenital obstruction of the ureter caused by ureteral valves in a 66-year-old male, namely, compression and constriction of the proximal part of the left ureter caused by valves (shown by the arrow) with a prominent hydronephrosis and formation of a diverticulum in the proximal part of the left ureter (After Kim et al. [52])
Ureteral pseudodiverticula can be considered a special type of ureteral diverticula (Fig. 2.5) or periglandular ureteritis (the term used by several authors) [42]. Ureteral pseudodiverticula (UPD) are most often found in men above 50 years old [43–48]. The actual UPD rate is not known. This is attributed to the impossibility to see UPD during EU. Hematuria is the most frequent manifestation which is followed by urological examination. The examination reveals diverticula and in most cases a concurrent infection and/or obstruction of the urinary tract.

Fig. 2.5
Pseudodiverticula of the left ureter in a retrograde ureterogram in case of ureteral valves (After Kim et al. [52])
As was mentioned above, UD are traditionally divided into two categories: congenital and acquired UD. Congenital (true) diverticula are usually solitary and contain all layers of the normal ureter wall, while the walls of acquired (false) UD consist only of the muscle layer. Histologic examination of multiple UPD reveals that these diverticula do not fall within any of the categories since such “outpouchings” do not consist of the complete ureter wall nor do they prolapse through the muscle layer. Since there is no certainty whether UPD are congenital or acquired, they are probably a metaplastic or hyperplastic reaction of the transitional epithelium which appears due to inflammation and may be part of cystic pyeloureteritis presentation. Actually, the combination of acquired diverticula with a stricture or defect of urinoexcretory system filling more likely means presence of a tumor.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


