Chapter 40 The spinal cord forms in three stages beginning in the third gestational week when the notochord induces surrounding ectoderm to differentiate into neuroectoderm.1 The first stage, neurulation, involves progression from neural plate to neural groove to neural tube.1 The notochord transforms into the nucleus pulposus of the intervertebral disks.2 The second stage, canalization, involves formation of cysts within the caudal cell mass that gradually coalesce and fuse to the distal neural tube to form the primitive spinal cord. The third stage, retrogressive differentiation, involves programmed cell death leading to regression of the primitive distal spinal cord to form the fetal conus, filum terminale, and ventriculus terminalis1,2 (Fig. 40-1). Figure 40-1 Embryological development of the spinal cord. The vertebral bodies develop from somites that have been converted through signaling molecules to form sclerotomes.3 The caudal and cranial portions of adjacent sclerotomes fuse to become single vertebral bodies. Failure of this process leads to congenital vertebral segmentation anomalies such as block or hemivertebrae (Fig. 40-2).4,5 Figure 40-2 Embryological development of the vertebra. Although 5% of humans have differing numbers of vertebrae, most often people have 7 cervical, 12 thoracic, and 5 lumbar vertebral bodies, as well as 5 sacral and 4 coccygeal segments.6 Running craniocaudal are the anterior and posterior longitudinal ligaments, supraspinous and interspinous ligaments, and ligamentum flavum. The arterial supply to the spinal cord is via the single, midline anterior spinal artery and the paired posterior spinal arteries. The anterior spinal artery originates from bilateral branches of the intradural segments of the vertebral arteries and courses along the ventral surface of the spinal cord. Similarly, the posterior spinal arteries arise from the intradural vertebral arteries, but course along the dorsal surface of the spinal cord.7 Radicular artery branches contribute to the cord arterial supply at multiple points. One particularly large branch, the artery of Adamkiewicz, typically enters the spinal canal between the T9 and T12 levels and can be recognized by its characteristic proximal hairpin turn.8 The indications for spine ultrasonography include screening neonates with multiple congenital anomalies, screening complicated dimples with skin stigmata, and evaluating soft tissue masses that suggest possible underlying closed (occult) spinal dysraphism, as well as determining the cause of failed lumbar puncture and localizing fluid for possible additional attempts at lumbar puncture.9,10 High-risk skin stigmata include atypical dimples (>5 mm) located above the gluteal crease (>2.5 mm from the anus), dimples in which the bottom cannot be visualized, and those with skin stigmata such as a hairy patch, hemangioma, a mound of soft tissue, skin tag, or tail.11 In anomalies requiring surgery and dimples draining cerebrospinal fluid, urgent MRI is the initial study of choice.12,13 Additionally, MRI is helpful to further characterize anomalies found on ultrasound and is best performed immediately prior to therapeutic intervention.9
Embryology, Anatomy, and Normal Findings
Embryology
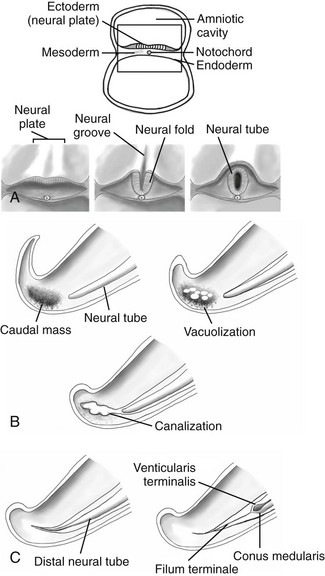
A, Neurulation schematic illustrates progression from neural plate to groove to neural tube. B, Canalization schematic depicts coalescence of cysts within the caudal cell mass that fuse to the distal neural tube. C, A retrogressive differentiation schematic reveals the process of programmed cell death forming the conus medullaris and filum terminale.
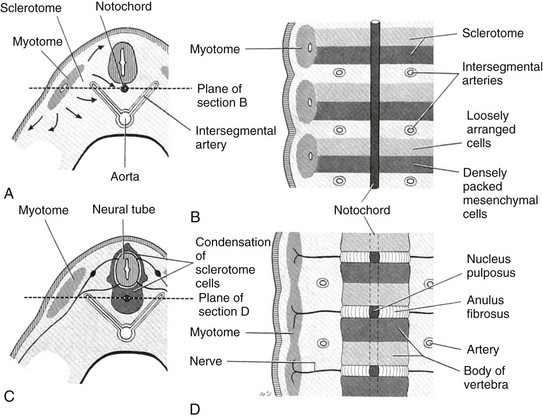
A, A partial transverse section through a 4-week embryo shows arrows indicating the spread of mesenchymal cells from the sclerotome region of the somite on the right. B, A diagrammatic frontal section of this embryo showing that the condensation of sclerotome cells around the notochord consists of a cranial area of loosely packed cells and a caudal area of densely packed cells. C, A partial transverse section through a 5-week embryo shows the condensation of sclerotome cells around the notochord and the neural tube, which forms a mesenchymal vertebra. D, A diagrammatic frontal section illustrates that the vertebral body forms from the cranial and caudal halves of two successive sclerotomes. The intersegmental arteries now cross the bodies of the vertebrae, and the spinal nerves lie between the vertebrae. The notochord is degenerating except in the intervertebral disk, where it persists as the nucleus pulposus. (From Moore KL. The developing human: clinically oriented embryology. 4th ed. Philadelphia: Saunders; 1988:338.)
Anatomy and Physiology
Normal Findings
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Embryology, Anatomy, and Normal Findings





