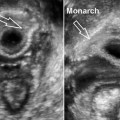
Fig. 10.1
Three-dimensional endorectal ultrasound performed with 2050 transducer (B-K Medical). Endometriosis lesion infiltrating the perirectal fat. The rectal layers are intact. (a) Axial plane, (b) coronal with axial plane. Two heterogeneous hypoechoic images in the left lateral quadrant compromising the perirectal fat (arrows). Mucus in the rectal lumen, outside the lesion site (artifacts)
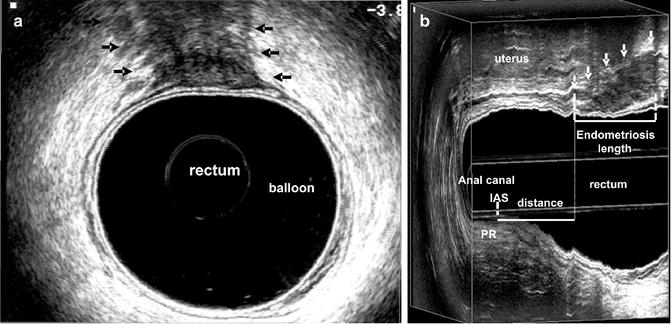
Fig. 10.2
Three-dimensional endorectal ultrasound performed with 2050 transducer (B-K Medical). Endometriosis lesion in the anterior quadrant infiltrating the rectal wall as far as the muscular propria (arrows). (a) Axial plane. Heterogeneous hypoechoic image compromising 20 % of rectal circumference (arrows). (b) Sagittal plane. The length of the endometriosis lesion and the distance between the distal infiltration edge and the proximal edge of the sphincter muscles (posterior quadrant) (arrows). IAS internal anal sphincter, PR puborectalis muscle
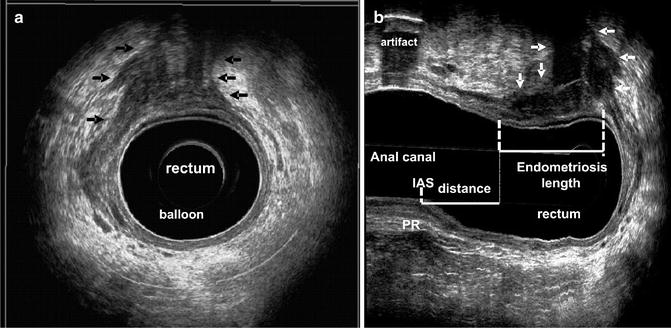
Fig. 10.3
Three-dimensional endorectal ultrasound performed with 2050 transducer (B-K Medical). Endometriosis lesion in the right anterior quadrant infiltrating the rectal wall as far as the muscular propria. (a) Axial plane. Heterogeneous hypoechoic image compromising 30 % of rectal circumference (arrows). (b) Sagittal plane. The length of the endometriosis lesion and the distance between the distal infiltration edge and the proximal edge of the sphincter muscles (posterior quadrant) (arrows). Mucus in the rectal lumen, outside the lesion site (artifacts). IAS internal anal sphincter, PR puborectalis muscle
10.3 Presacral Neoplasia
Perirectal neoplasia is most often located in the retrorectal space and may be of varied etiology. Half the cases are congenital and two thirds are cystic in nature [8, 9]. It tends to affect young female adults but is uncommon in infants. Teratoma is the most frequently observed form in pediatric patients and contains fat or calcifications in 50 % of cases [9, 10].
A wide variety of cystic lesions occur in the retrorectal space, and most are congenital. They are classified as epidermoid cysts, dermoid cysts, enteric cysts (tailgut cysts and cystic rectal duplication), and neurenteric cysts according to their origin and histopathologic features [11]. Anorectal ultrasound may show specific signs and characteristics of the lesion (anechoic area with circular or oval shape, regular margin, and with reinforcement of posterior wall) but the diagnosis remains histopathologic. Ultrasonographic imaging is useful in the evaluation of size, type of lesion (mixed cystic and solid components), and relation with the rectal wall and the sphincter muscles (Figs. 10.4a, b and 10.5a–c).
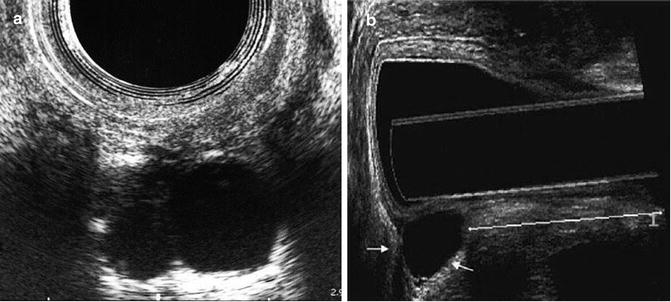
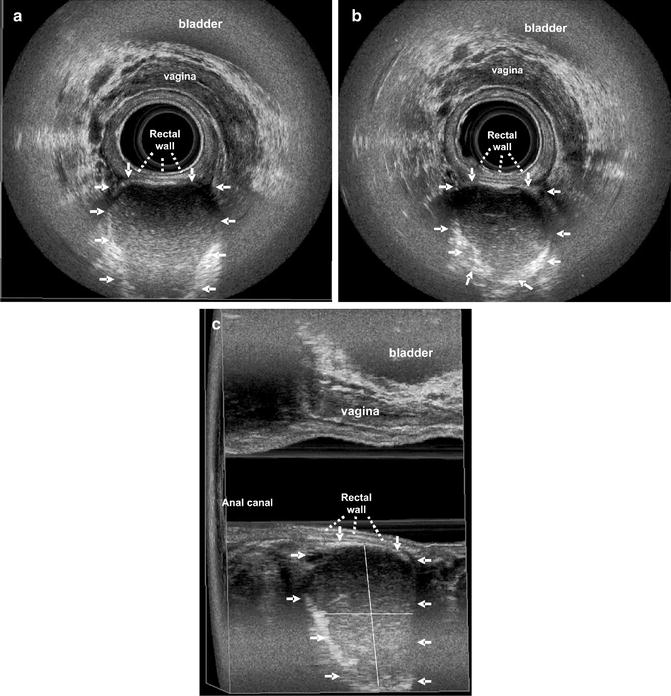
Fig. 10.4
Three-dimensional endorectal ultrasound performed with 2050 transducer (B-K Medical). Female patient. Presacral developmental cyst. The lesion appears as a well-circumscribed, hypoechoic area with posterior reinforcement. The layers of the rectal wall are preserved. (a) Axial plane. (b) Sagittal plane. Lesion size (longitudinal length and the depth)
Fig. 10.5
Three-dimensional endorectal ultrasound performed with 2050 transducer (B-K Medical). Female patient. Presacral cystic lesion located at the level of lower rectum with regular outline and without adherence to the rectal wall (arrows). The rectal wall is intact. (a, b) Axial plane. Mixed echogenicity lesion (arrows). (c) Sagittal with diagonal planes. A well-circumscribed (hyperechogenic line that surrounds the lesion) and unilocular cystic lesion. Lesion size (longitudinal length and the depth)
Perirectal neoplasia appears with different characteristics: as a unilocular or multilocular retrorectal lesion, sometimes a hypoechoic area (cystic) or as an area of mixed echogenicity/heterogeneous image, due to mucoid material or inflammatory debris or solid component, usually with regular outline and not adhering to the rectal wall. In large lesion, an anorectal displacement or stenosis may be visualized due to extrinsic compression. It is important to define the rectal wall invasion or a communication between the cyst and the anorectal lumen (Fig. 10.6a–c).
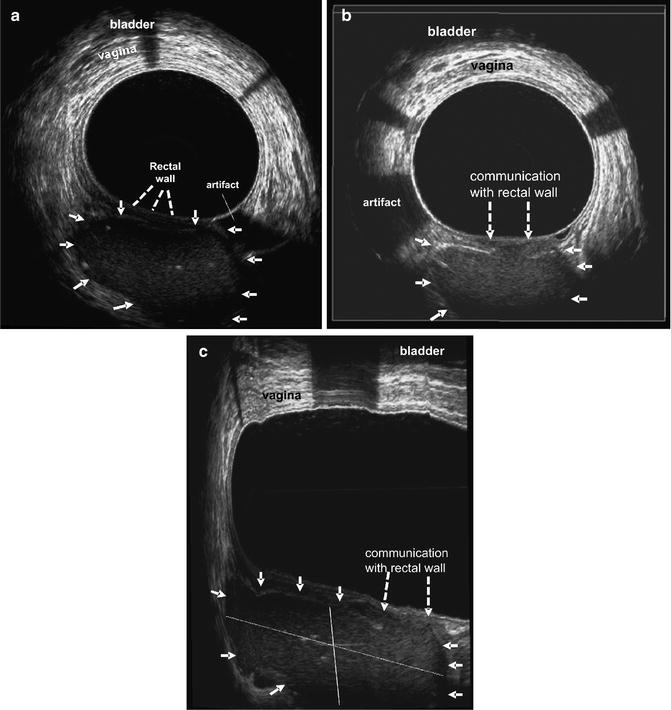
Fig. 10.6
Three-dimensional endorectal ultrasound performed with 2050 transducer (B-K Medical). Female patient. Cystic lesion in the presacral space at the level of lower rectum. There is a contiguous (communication) area with rectal wall. (a) Axial plane. In this position, the lesion appears with mixed echogenicity, with regular outline and without adherence to the rectal wall (arrows). The rectal wall is intact. (b) Axial plane. The image shows the area of the cystic lesion, which communicates with the rectal wall (interrupted arrows). (c) Sagittal plane. The hyperechogenic line that surrounds the lesion (arrows) is interrupted (small area) and there is a communication with rectal wall (interrupted arrows). Lesion size (longitudinal length and the depth)
10.4 Rare Tumors
10.4.1 Rectal Leiomyoma and Leiomyosarcoma
Leiomyoma is a benign mesenchymal neoplasm that usually develops where smooth muscle is present. This lesion is rare, except in the esophagus and rectum. Only 3 % of these smooth muscle tumors arising from colon are gastrointestinal leiomyomas and constitute about 0.1 % of rectal tumors [12, 13
 Three-Dimensional Endoanal Ultrasonography of the Anorectal Region
Three-Dimensional Endoanal Ultrasonography of the Anorectal Region
 Endovaginal Urethra and Bladder Imaging
Endovaginal Urethra and Bladder Imaging
 Emerging Imaging Technologies and Techniques
Emerging Imaging Technologies and Techniques
 3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
 Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
 2D/3D Endovaginal and Endoanal Instrumentation and Techniques
2D/3D Endovaginal and Endoanal Instrumentation and Techniques




Related posts:
Three-Dimensional Endoanal Ultrasonography of the Anorectal Region
Endovaginal Urethra and Bladder Imaging
Emerging Imaging Technologies and Techniques
3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
2D/3D Endovaginal and Endoanal Instrumentation and Techniques
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
