Fig. 9.1
High-multifrequency (9-16MHz), 360° rotational mechanical probe (type 2050, BK Medical, Herlev, Denmark
Fig. 9.2
Schematic illustration of the technique of three-dimensional endoanal ultrasonography performed by 2050 transducer (B-K Medical)
Before the probe is inserted into the anus, a digital rectal examination should be performed. If there is an anal stenosis, the finger can check to determine whether it will allow easy passage of the probe. A gel containing condom is placed over the probe, and a thin layer of water-soluble lubricant is placed on the exterior of the condom. Any air interface will cause a major interference pattern. The patient should be instructed before the examination that no pain should be experienced. Under no circumstances should force be used to advance the probe. During examination, the patient may be placed in the dorsal lithotomy, in the left lateral or in the prone position. However, irrespective of the position, the transducer should be rotated so that the anterior aspect of the anal canal is superior (12 o’clock) on the screen, right lateral is left (9 o’clock), left lateral is right (3 o’clock), and posterior is inferior (6 o’clock). The length of recorded data should extend from the upper aspect of the “U”-shaped sling of the puborectalis (PR) to the anal verge.
9.3 Endosonographic Anatomy of the Normal Anal Canal
On ultrasound five hypoechoic and hyperechoic layers can be seen in the normal anal canal [6]. The ultrasonographer must have a clear understanding of what each of these five lines represent anatomically (Fig. 9.3):
Fig. 9.3
(a) Normal ultrasonographic five-layer structure of the mid-anal canal. Axial image obtained by 2050 transducer (B-K Medical); (b) schematic representation
1.
The first hyperechoic layer, from inner to outer, corresponds to the interface of the transducer with the anal mucosal surface.
2.
The second layer represents the subepithelial tissues and appears moderately reflective. The mucosa as well the level of dentate line is not visualized. The muscularis submucosae ani can be sonographically identified in the upper part of the anal canal as a low reflective band.
3.
The third hypoechoic layer corresponds to the internal anal sphincter (IAS). The sphincter is not completely symmetric, either in thickness or termination. It can be traced superiorly into the circular muscle of the rectum, extending from the anorectal junction to approximately 1 cm below the dentate line. In older age groups, the IAS loses its uniform low echogenicity, which is characteristic of smooth muscle throughout the gut, to become more echogenic and inhomogeneous in texture.
4.
The fourth hyperechoic layer represents the longitudinal muscle (LM). It presents a wide variability in thickness and not always is distinctly visible along the entire anal canal. The LM appears moderately echogenic, which is surprising as it is mainly smooth muscle; however, an increased fibrous stroma may account for this. In the intersphincteric space, the LM conjoins with striated muscular fibers from the levator ani, particularly the puboanalis, and a large fibroelastic element derived from the endopelvic fascia to form the “conjoined longitudinal layer” (CLL) (Fig. 9.4). Its fibroelastic component, permeating through the subcutaneous part of the external anal sphincter (EAS), terminates in the perianal skin.
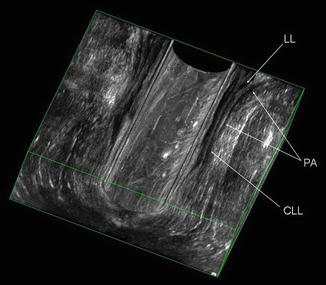
Fig. 9.4
Coronal image of the anal canal from three-dimensional reconstruction obtained by 2050 transducer (B-K Medical). The puboanalis (PA) joins the longitudinal muscle layer (LL) of the rectum to form the conjoined longitudinal layer (CLL)
5.
The fifth mixed echogenic layer corresponds to the EAS. The EAS is made up of voluntary muscle that encompasses the anal canal. It is described as having three parts: (1) the deep part is integral with the PR. Posteriorly there is some ligamentous attachment. Anteriorly some fibers are circular and some decussate into the deep transverse perinei; (2) the superficial part has a very broad attachment to the underside of the coccyx via the anococcygeal ligament. Anteriorly there is a division into circular fibers and a decussation to the superficial transverse perinei; (3) the subcutaneous part lies below the IAS.
Ultrasound imaging of the anal canal can be divided into three levels of assessment in the axial plane (upper, middle, and lower levels) referring to the following anatomical structures (Fig. 9.5) [6]:
Fig. 9.5
(a) Three levels of assessment of the anal canal in the axial plane. Scan obtained by 2050 transducer (B-K Medical). EAS external anal sphincter, IAS internal anal sphincter, PR puborectalis; (b) three-dimensional reconstruction on the coronal plane
1.
Upper level: the sling of the puborectalis (PR), the deep part of the EAS, and the complete ring of IAS
2.
Middle level: the superficial part of the EAS (complete ring), the CLL, the IAS (complete ring), and the transverse perinei muscles
3.
Lower level: the subcutaneous part of the EAS
The anal canal length is the distance measured between the proximal canal, where the PR is identified, and the lower border of the subcutaneous EAS. It is significantly longer in male than in female, as a result of a longer EAS, whereas there is no difference in PR length. The anterior part of the EAS differs between genders and anatomic studies showed that this difference is already present in fetal age. In males, the EAS is symmetrical at all levels; in females, it is shorter anteriorly, and there is no evidence of anterior ring high in the canal. In examining a female subject, the ultrasonographic differences between the natural gaps (hypoechoic areas with smooth, regular edges) and sphincter ruptures (mixed echogenicity, due to scarring, with irregular edges) occurring at the upper anterior part of the anal canal must be kept in mind. Three-dimensional longitudinal images are particularly useful to assess these anatomic characteristics of the EAS (Fig. 9.6) [7–10]. Williams et al. [7] reported that the anterior EAS occupied 58 % of the male anal canal compared with 38 % of the female canal (P < 0.01). In female the PR occupied a significantly larger proportion of the canal than in male (61 % vs. 45 %; P = 0.02). There was no difference in the length of the IAS between male and female (34.4 vs. 33.2 mm) or the proportion of the anal canal that it occupied (67 % vs. 73 %; P = 0.12).
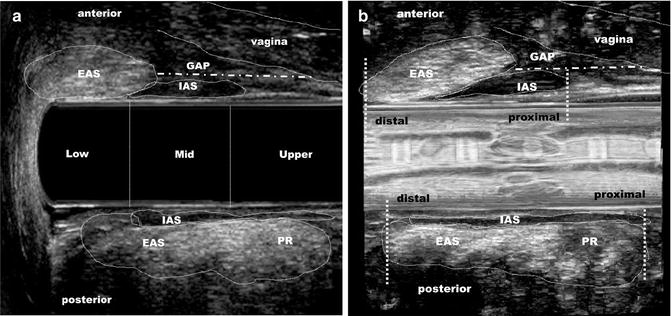
Fig. 9.6
(a) Female anal canal anatomic configuration. Three-dimensional reconstruction on the sagittal plane shows the asymmetrical shape of the anal canal and the positions of anal sphincters. The anterior anal canal (EAS and IAS) starts and ends more distally and the posterior anal canal (PR-EAS and IAS starts) starts and ends more proximally. EAS external anal sphincter, IAS internal anal sphincter, PR puborectalis muscle, GAP the area in the anterior quadrant without striated muscle, measured from the proximal edge of the posterior PR to the proximal edge of the anterior EAS; (b) render mode
Normal values for sphincter dimensions differ between techniques [6]. The importance to define the true values of sphincter muscle thickness is not very relevant, because the purpose of measuring anal sphincters is to distinguish a normal vs. abnormal measurement, regardless of the absolute values. Measurement should be taken at the 3, 6, 9, and 12 o’clock positions in the midlevel of the anal canal. The thickness of IAS varies from 1.8 ± 0.5 mm and increases with age owing the presence of more fibrous tissue as the absolute amount of muscle decreases, measuring 2.4–2.7 mm <55 years and 2.8–3.5 mm >55 years. Any IAS >4 mm thick should be considered abnormal whatever the patient’s age; conversely a sphincter of 2 mm is normal in a young patient, but abnormal in an elderly one. The LM is 2.5 ± 0.6 mm in males and 2.9 ± 0.6 mm in females. The average thickness of the EAS is 8.6 ± 1.1 mm in males and 7.7 ± 1.1 mm in females. However, endosonography largely overestimates the size of the EAS due to its failure to recognize and separate the LM. Frudinger et al. [11] reported a significant negative correlation of the EAS thickness with the patient’s age at all anal canal levels. In particular, the anterior EAS part was found significantly thinner in older subjects.
Multiplanar EAUS has enabled detailed longitudinal measurement of the components of the anal canal (Figs. 9.6 and 9.7). Williams et al. [7] reported that the anterior EAS was significantly longer in men than women (30.1 vs. 16.9 mm; P < 0.001). There was no difference in the length of the PR between men and women, indicating that the gender difference in anal canal length is solely due to the longer male EAS. The IAS did not differ in length between males and females. Regadas et al. [8] demonstrated the asymmetrical shape of the anal canal and also confirmed that the anterior EAS was significantly shorter in female. West et al. [12] reported similar results, with IAS and EAS volumes found larger in males than in females.
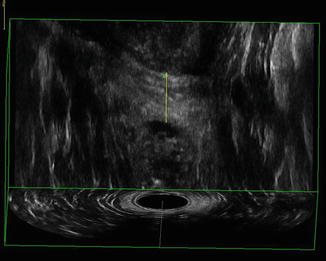
Fig. 9.7
Three-dimensional endoanal ultrasonography performed by 2050 transducer (B-K Medical). Measurement of the anterior length of the external sphincter in the coronal plane
Regardless of the absolute values of the anal sphincter, the most relevant utility of EAUS applies in the detection of localized sphincter defects, where its benefit has been proved [13, 14]. It has been suggested that measuring sphincter thickness is important when EAUS cannot depict any sphincter damage to exclude diffuse structural sphincter changes associated with idiopathic fecal incontinence, passive fecal incontinence, or obstructive defecation disorders. A postulated association between manometric function of the sphincters and their sonographic appearance, however, remained controversial in the literature. Some authors have found no correlation between muscle thickness and muscle performance, neither resting nor squeeze pressure. Scanning anal sphincter muscle may allow for determination of their integrity, but not for their morphometric properties.
9.4 Endosonographic Anatomy of the Rectum
The normal rectum is 11–15 cm long and has a maximum diameter of 4 cm. It is continuous with the sigmoid colon superiorly at the level of the third sacral segment and courses inferiorly along the curve of the sacrum to pass through the pelvic diaphragm and become the anal canal. It is surrounded by fibrofatty tissue that contains blood vessels, nerves, lymphatics, and small lymph nodes. The superior one-third is covered anteriorly and laterally by the pelvic peritoneum. The middle one-third is only covered with peritoneum anteriorly, where it curves anteriorly onto the bladder in the male and onto the uterus in the female. The lower one-third of the rectum is below the peritoneal reflection and is related anteriorly to the bladder base, ureters, seminal vesicles, and prostate in the male and to the lower uterus, cervix, and vagina in the female.
The rectal wall consists of five layers surrounded by perirectal fat or serosa [15]. On ultrasound the normal rectal wall is 2–3 mm thick and is composed of a five-layer structure. Good visualization depends on maintaining the probe in the center lumen of the rectum and having adequate distension of a water-filled latex balloon covering the transducer to achieve good acoustic contact with the rectal wall. It is important to eliminate all bubbles within the balloon to avoid artifacts that limit the overall utility of the study. The rectum can be of varying diameters and therefore the volume of water in the balloon may have to be adjusted intermittently. The five layers represent (Fig. 9.8):
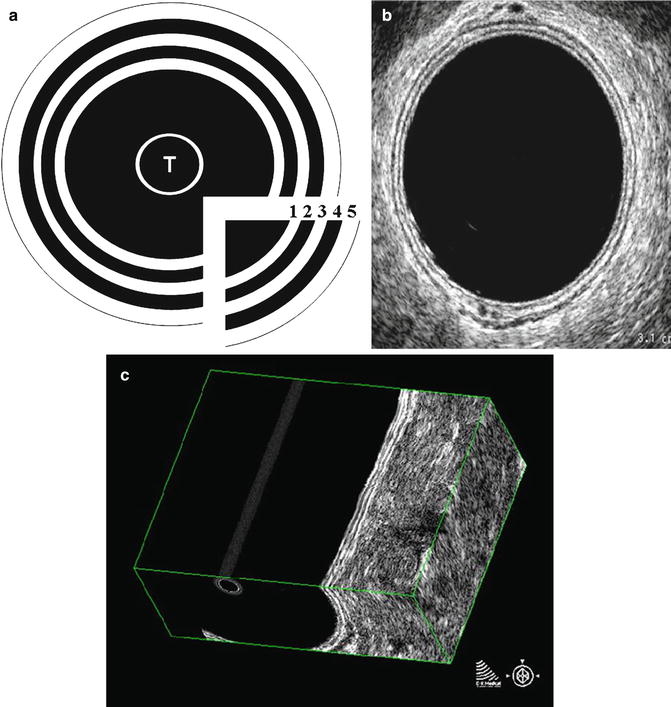
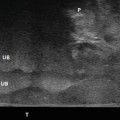
Fig. 9.8
(a) Schematic ultrasound representation of the rectal wall (T transducer); (b) the five layers in the axial plane correspond to (1) acoustic interface with mucosal surfaces, (2) mucosa, (3) submucosa, (4) muscularis propria, and (5) serosa/perirectal fat interface; (c) three-dimensional reconstruction of the rectal wall in the coronal plane. Scans obtained by 2050 transducer (B-K Medical)
1.
The first hyperechoic layer: the interface of the balloon with the rectal mucosal surface
2.
The second hypoechoic layer: the mucosa and muscularis mucosae
3.
The third hyperechoic layer: the submucosa
4.
The fourth hypoechoic layer: the muscularis propria (in rare cases seen as two layers: inner circular and outer longitudinal layer)
5.
The fifth hyperechoic layer: the serosa or the interface with the fibrofatty tissue surrounding the rectum (mesorectum). The mesorectum contains blood vessels, nerves, and lymphatics and has an inhomogeneous echo pattern. Very small, round to oval, hypoechoic lymph nodes should be distinguished from blood vessels which also appear as circular hypoechoic structures.
Endorectal US allows an accurate visualization of all pelvic organs adjacent to the rectum: the bladder, seminal vesicles, and prostate in male and the uterus, cervix, vagina, and urethra in female. Intestinal loops can also easily identified as elongate structures.
9.5 Clinical Application of 3D Endoanal/Endorectal Ultrasound
Clinical applications of pelvic floor ultrasonography [1] for both anatomical assessment and evaluation of function of posterior compartment disorders are reported in detail below.
9.5.1 Fecal Incontinence
Fecal incontinence (FI) is defined as the involuntary loss of feces (liquid or solid stool) and anal incontinence is defined as the complaint of involuntary loss of flatus or feces [13]. A meta-analysis revealed a rate of 11–15 % in the general population, although it may perhaps be underestimated [16]. Intact musculature including the PR, IAS, and EAS are prerequisites for fecal control, as is a functioning nerve supply to these muscles. Other factors contributing to FI include stool consistency, rectal sensitivity and capacity, and the anorectal angle (ARA). Any impairment to one or more of these factors may result in FI. Anal sphincter defects and pudendal nerve injury can occur during vaginal delivery and are by far the most common causes of FI, consequently making this problem more prevalent in women [16].
In patients with FI, therefore, it is fundamental to establish the underlying pathophysiology in order to choose the appropriate therapy (dietary or medications, biofeedback, sphincter repair, artificial bowel sphincter, graciloplasty, sacral nerve stimulation, injection of bulking agents). EAUS has become the gold standard for the morphological assessment of the anal canal [13, 14]. It can differentiate between incontinent patients with intact anal sphincters and those with sphincter lesions (defects, scarring, thinning, thickening, and atrophy). Tears are defined by an interruption of the circumferential fibrillar echo texture. Scarring is characterized by loss of normal architecture, with an area of amorphous texture that usually has low reflectivity. The operator should identify if there is a combined lesion of the IAS and EAS or if the lesion involves just one muscle. The number, circumferential (radial angle in degrees or in hours of the clock site), and longitudinal (proximal, distal, or full length) extension of the defect should be also reported. In addition, 3D EAUS allows to measure length, thickness, area of sphincter defect in the sagittal and coronal planes, and volume of sphincter damage (Figs. 9.9, 9.10, 9.11, and 9.12) [5].
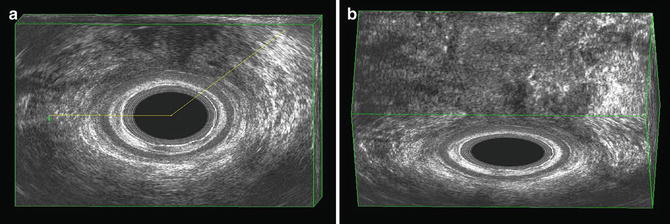
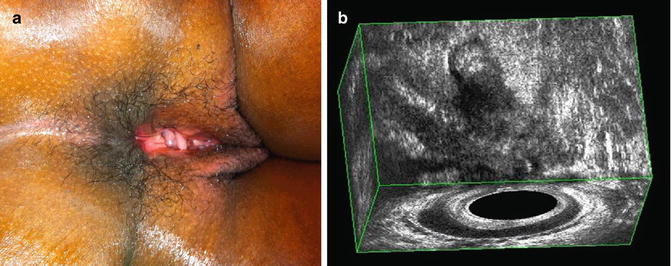

Fig. 9.9
(a) Internal anal sphincter lesion between 3 o’clock and 9 o’clock position following a left lateral internal sphincterotomy for fissure. (b) Anterior internal anal sphincter damage demonstrated with three-dimensional reconstruction in the sagittal plane. Scans obtained by 2050 transducer (B-K Medical)
Fig. 9.10
(a) External sphincter lesion between 9 o’clock and 1 o’clock position due to obstetric trauma. (b) Anterior external anal sphincter damage demonstrated with three-dimensional reconstruction in the coronal plane. Scans obtained by 2050 transducer (B-K Medical)
Fig. 9.11
(a) Fourth-degree anal sphincter lesion due to obstetric trauma. (b) Three-dimensional reconstruction demonstrates the combined anterior damage of the internal and external anal sphincters in the coronal and axial planes. Scans obtained by 2050 transducer (B-K Medical)
Fig. 9.12
External anal sphincter atrophy. Three-dimensional reconstruction in the coronal plane demonstrates a short anterior length (6.6 mm) of the external sphincter. Scans obtained by 2050 transducer (B-K Medical)
Using multiplanar EAUS, two scoring systems have been proposed to define the severity of the sphincter damage. Starck et al. [17] introduced a specific score, with 0 indicating no defect and 16 corresponding to a defect >180° involving the whole length and depth of the sphincters. Recently, Norderval et al. [18] reported a simplified system for analyzing defects, including fewer categories than the Starck score and not recording partial defects of the IAS. A maximal score of 7 denotes defects in both the EAS and the IAS exceeding 90° in the axial plane and involving more than half of the sphincter length. Both systems showed good intraobserver and interobserver agreement in classifying anal sphincter defects.
The presence of a sphincter defect, however, does not necessarily mean that it is the cause of FI, as many people have sphincter lesions without having symptoms of incontinence [19]. On the other hand, patients with FI and an apparent intact sphincter can have muscle degeneration, atrophy, or pudendal neuropathy. EAUS has an important role in detecting clinically occult anal sphincter injuries after a vaginal delivery [20]. In a meta-analysis of 717 vaginal deliveries, Oberwalder et al. [21] found an incidence of occult sphincter damage of 26.9 % among a sample of 462 primiparous women and a rate of 8.5 % new defects in the group of 255 multiparas. In one-third of these (29.7 %), postpartum sphincter damage was symptomatic. As shown in this meta-analysis, the probability that postpartum FI will be associated with anal sphincter defect is 77–83 %. This analysis included five studies where EAUS was the only imaging technique used. In another study, Oberwalder et al. [22] reported that FI related to sphincter lesions is likely to occur even in an elderly population of women who experienced vaginal deliveries earlier in life. They found that 71 % of women with late-onset FI (median age 61.5 years) had occult sphincter defects on EAUS.
Ultrasonographic imaging is useful to evaluate the result of treatments. Starck et al. [23] reported that the extent of endosonographic EAS defects after primary repair of obstetric sphincter tears increased over time and was related to FI. Scheer et al. [24] have demonstrated the value of EAUS and manometry in counselling women who previously sustained obstetric tears. Based on specific selection criteria, the majority of women delivered vaginally without deterioration in anal sphincter morphology and function or quality of life. Savoye-Collet et al. [25] noted improvement in FI in 86 % of patients in whom EAUS documented closure of the EAS defect after anterior sphincter repair. In contrast, patients who had a persistent defect in the EAS still had significant FI. Dobben et al. [26] also found that patients with a persistent ultrasonographic EAS defect had a worse clinical outcome than those without an EAS defect.
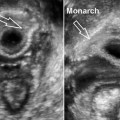
Using 3D-EAUS, de la Portilla et al. [27] demonstrated that all the implants of silicone to treat FI were properly located in the intersphincteric space 3 months after injection. At 24 months, 75 % of implants were still properly located. They found that the continence deterioration suffered by most patients after the first year from the injection was not related to the localization and number of implants the patient had (Fig. 9.13).
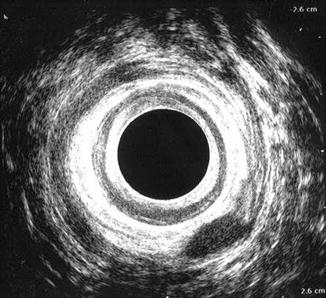
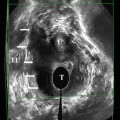
Fig. 9.13
Failure after bulking agent injection. Postoperative assessment with endoanal ultrasound demonstrated that the agent was positioned outside the external sphincter and not in the intersphincteric space. Scans obtained by 2050 transducer (B-K Medical)
9.5.2 Obstructed Defecation and Posterior Vaginal Wall Prolapse
Anorectal outlet obstruction, also known as obstruction defecation syndrome (ODS), is a pathological condition due to a variety of causes and is characterized by an impaired expulsion of the bolus after calling to defecate [13]. Patients complain of different symptoms, including incomplete evacuation with or without painful effort, unsuccessful attempts with long periods spent in bathroom, return visit to the toilette, use of perineal support, manual assistance (insertion of finger into the vagina or anal canal), straining, and dependence on enema and/or laxatives. Other symptoms are pain at defecation; extreme straining to defecate; extended time at the toilet; perineal pain/discomfort when standing; feeling of incomplete evacuation; fragmented defecation; vaginal, perineal, or rectal digitation; use of laxatives or enemas; and fecal incontinence [13]. These symptoms often lead to a poor quality of life. Prevalence of the entire spectrum of constipation, of which ODS is part, accounts for 14.7 % in the US adult population while the true prevalence of ODS among the population is not known even if the feeling is that it is underestimated.
After ruling out pelvic and rectal tumor, the main distinction in the pathogenesis of ODS is between functional and mechanical causes. Failure to release the anal sphincters or paradoxical contraction of the PR muscle are considered the main and most frequent functional causes of ODS. In these patients, biofeedback can achieve reactivation of the inhibitory capacity of all pelvic floor muscles involved in defecation, with an improvement in symptoms of 50 %. The most relevant mechanical causes of ODS are rectocele, rectal intussusception, enterocele, genital prolapse, and descending perineum. It is fundamental to distinguish between rectal causes (rectocele and intussusception) and extrarectal causes (enterocele, genital prolapse, and descending perineum).
In recent years, alternatives to defecography, such as dynamic MRI and dynamic ultrasonography, have been developed for the evaluation of pelvic floor dysfunctions, with good correlation and the advantage of showing the entire pelvis [28–38]. Studies using dynamic ultrasound with different types of transducers (convex, endfire, biplanar probes) and different techniques (translabial, transperineal, introital ultrasound) have produced findings consistent with defecography to assess patients with ODS [31–38]. Murad-Regadas et al. [35
 Endovaginal Imaging of Vaginal Implants
Endovaginal Imaging of Vaginal Implants
 Endovaginal Urethra and Bladder Imaging
Endovaginal Urethra and Bladder Imaging
 Emerging Imaging Technologies and Techniques
Emerging Imaging Technologies and Techniques
 3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
 Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
 2D/3D Endovaginal and Endoanal Instrumentation and Techniques
2D/3D Endovaginal and Endoanal Instrumentation and Techniques




Related posts:
Endovaginal Imaging of Vaginal Implants
Endovaginal Urethra and Bladder Imaging
Emerging Imaging Technologies and Techniques
3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
2D/3D Endovaginal and Endoanal Instrumentation and Techniques
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
