Fig. 8.1
Left Bartholin gland cyst. Axial view with 360° endovaginal ultrasound probe. A anus, BG Bartholin gland, LA levator ani muscle, T transducer. © Shobeiri
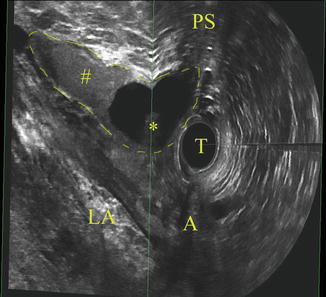
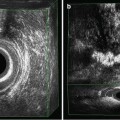
Fig. 8.2
Right Bartholin gland cyst. Axial and sagittal view with 360° endovaginal probe. Internal echo can be seen in cyst. In sagittal view cephalad extension of cyst can be evaluated. A anus, LA levator ani muscle, PS pubic symphysis, T transducer, # internal echo of cyst, * Bartholin gland cyst. © Shobeiri
8.2.3 Skene Gland Cyst/Abscess
Paraurethral Skene glands are considered the homologue of the prostate in females [16, 17]. Controversy exists on the function of Skene’s glands, their role in sexual function, female orgasm and ejaculation, and even their anatomy. Infection in these glands was described with gonorrheal infection in 1672 by Regnier de Graaf (1641–1693), which was long before Skene described them in 1880. Asymptomatic cysts of the duct or gland are uncommon and when infection occurs can cause pain, dysuria, vaginal discharge, and dyspareunia. On examination a palpable painful mass is present next to the distal urethra and purulent material can be expressed from the ductal orifice. Skene’s abscesses can be distinguished from urethral diverticulum, which is usually more proximal and communicates with the urethra through a diverticular orifice. When doubt exists, imaging with positive pressure urography using a Trattner’s catheter, ultrasound, or MRI can be helpful [18].
3D Endovaginal Ultrasound Appearance of Skene Gland Cyst
Skene glands are group of tubular glands that lie on the vaginal surface of the urethra. These paraurethral glands empty into the lumen at several points on the dorsal surface of the urethra; the majority of them are located in the middle to distal urethra, near the 3 o’clock and 9 o’clock positions [19]. Two prominent openings on the inner aspects of the external urethral orifice can be seen when the orifice is open. Obstruction of their terminal duct can result in cyst formation.
They represent smooth margins on ultrasound images. Depending on its contents, the cyst may show no internal echoes or echoes may diffusely line the interior of the cysts (Figs. 8.3 and 8.4).
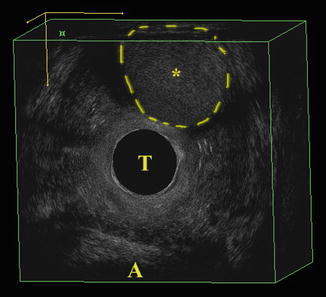
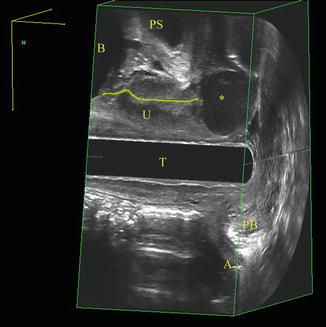
Fig. 8.3
Skene gland mass. Axial view with 360° endovaginal probe. A anus, T transducer, * Skene gland mass. © Shobeiri
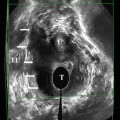
Fig. 8.4
Skene gland cyst. Midsagittal view with 360° endovaginal probe. A anus, B bladder, PB perineal body, PS pubic symphysis, T transducer, U urethra, * Skene gland cyst. © Shobeiri
8.2.4 Urethral Diverticulum
Urethral diverticulum in women may be more common than has been suspected and should be excluded in patients with chronic irritative voiding symptoms, post void dribbling, or dyspareunia. The pathogenesis of this condition is poorly understood, and these lesions represent a spectrum of disorders ranging from isolated sub urethral cysts to herniation of the urethral lining into the vaginal mucosa. Urethral diverticula usually are small, varying from 3 mm to 3 cm in diameter. Although most diverticula lie posterior to the urethra, they also can be located laterally or anteriorly or even partially or completely surround the urethra (saddle diverticulum). Accurate diagnosis is based on history and clinical evaluation. Perineal ultrasound and MRI have been used for diagnosis. A diverticulum may fill during the voiding phase of urography or cystourethrography, presenting as a well-contained fluid collection adjacent to the urethra. Assessing urethral diverticula by sonography was first introduced by Lee and Keller [20]. Ultrasonography can be used to help differentiate solid from cystic sub urethral masses, to identify stones within diverticula, and to visualize intraluminal masses (e.g., carcinoma, nephrogenic adenoma, mesonephric adenocarcinoma) [21].
3D Endovaginal Ultrasound Appearance of Urethral Diverticulum
The majorities of urethral diverticula are located in the middle third of the urethra and involve the posterolateral wall [22]. Ultrasound shows a relatively echo-free cavity adjacent to the urethra with an orifice that communicates with the urethral lumen; it also may demonstrate inflammatory debris and/or surrounding inflammatory edema. Given that urethral diverticulum is very common, clinical acuity is needed to differentiate it from the other conditions (Figs. 8.5a, b and 8.6).
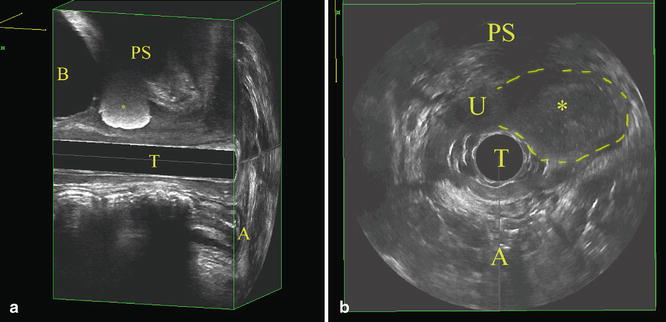
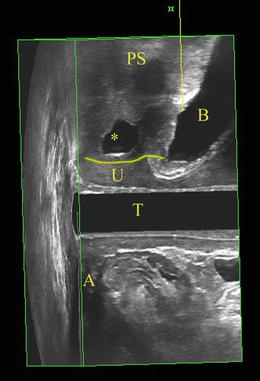
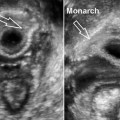
Fig. 8.5
(a) Left midsagittal view with 360° endovaginal probe of periurethral bulking agent at vesicourethral junction. A anus, B bladder, PS pubic symphysis, T transducer, * periurethral bulking material. © Shobeiri. (b) Axial view of a periurethral mass masquerading as a diverticulum. A anus, PS pubic symphysis, T transducer, * left periurethral mass with indistinct borders is outlined. © Shobeiri
Fig. 8.6
Urethral diverticulum anterior to the urethra seen at midsagittal view with 360° endovaginal probe. This patient’s complaint was pain and a palpable mass was not evident by physical examination. A anus, B bladder, PS pubic symphysis, T transducer, U urethral, * anterior urethral diverticulum. © Shobeiri
8.2.5 Gartner Duct Cyst
The distal mesonephric ducts in the female are resorbed but may persist as vestigial remnants in the anterolateral vaginal wall down to the hymen (Gartner’s duct cysts) and between the layers of the broad ligament (paraovarian cysts). These cysts are usually small and asymptomatic and have been reported to occur in as many as 1 % of all women [23, 24]. Because the ureteral bud also develops from the Wolffian duct, it is not surprising that Gartner duct cysts have been associated with ureteral and renal abnormalities in addition to associated anomalies of the female genital tract [25–28]. Ultrasonography of the upper and lower urinary tract is a noninvasive useful initial investigation. The Gartner duct cysts can be elusive and result in varied fistulas, including urethrovaginal fistulas [29].
Gartner duct cysts can have varied clinical presentations and 3D EVUS characteristics.
3D Endovaginal Ultrasound Appearance of Gartner Duct Cyst
Gartner’s duct cysts will usually be incidental findings during pelvic ultrasonography. Of developmental origin, they may present anywhere along the lateral aspect of the female genital tract. When the cysts are of paraovarian origin, they will mimic other fluid-filled adnexal masses, and no specific diagnosis can be made. When alongside the vagina or cervix, however, their ultrasonographic appearance is probably characteristic (Figs. 8.7 and 8.8).
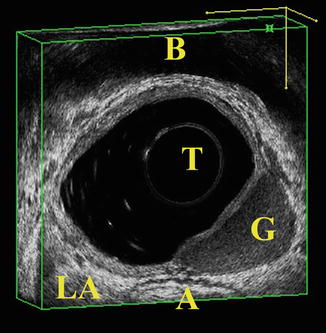
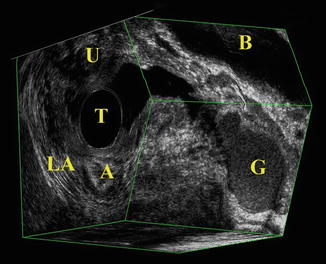
Fig. 8.7
Gartner duct cyst. Axial view with 360° endovaginal probe. A anus, B bladder, G Gartner duct cyst, LA levator ani muscle, T transducer. © Shobeiri
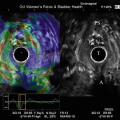
Fig. 8.8
Gartner duct cyst. Axial and sagittal view with 360° endovaginal probe. A anus, B bladder, G Gartner duct cyst, LA levator ani muscle, T transducer, U urethra. © Shobeiri
8.2.6 Leiomyoma of Vagina
Although uterine fibroids are common uterine benign neoplasms worldwide, and many treatment options exist for them, vaginal fibroid reports are scarce in the literature [30]. The boundaries of such mesodermal tumors are difficult to delineate, but most of the tumors are benign. Even recurrence does not signify malignant alteration. Vaginal leiomyoma presenting as a mass is most often diagnosed clinically and removed during surgery. An uncommon presentation may necessitate imaging studies. The lesion described can have MRI and ultrasound features similar to its uterine counterpart.
3D Endovaginal Ultrasound Appearance of Leiomyoma
Vaginal leiomyoma has variable consistency and can be cystic, semi-cystic, or solid. The ultrasound reveals the heterogeneous echo texture consistent with myomata (Fig. 8.9). The leiomyoma can occur anywhere along the vaginal tract; however the condition is very uncommon.
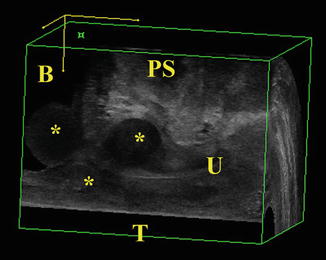
Fig. 8.9
Periurethral and endovesical leiomyoma. Midsagittal view with 180° endovaginal probe. Anterior compartment is visualized in this ultrasound image. B bladder, PS pubic symphysis, T transducer, U urethra, * leiomyoma. © Shobeiri
8.2.7 Malignant Vaginal Masses
Carcinoma of the vagina is uncommon, occurring in less than 2 % of patients with gynecologic malignancies. The most common histologic type of primary vaginal tumor is squamous carcinoma. As with cervical intraepithelial neoplasia and carcinoma, the human papilloma virus is probably responsible for the majority of vaginal carcinomas. Plentl and Friedman [31
 Three-Dimensional Endoanal Ultrasonography of the Anorectal Region
Three-Dimensional Endoanal Ultrasonography of the Anorectal Region
 Endovaginal Urethra and Bladder Imaging
Endovaginal Urethra and Bladder Imaging
 Emerging Imaging Technologies and Techniques
Emerging Imaging Technologies and Techniques
 3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
 Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
 2D/3D Endovaginal and Endoanal Instrumentation and Techniques
2D/3D Endovaginal and Endoanal Instrumentation and Techniques




Related posts:
Three-Dimensional Endoanal Ultrasonography of the Anorectal Region
Endovaginal Urethra and Bladder Imaging
Emerging Imaging Technologies and Techniques
3D Endovaginal Ultrasound Imaging of the Levator Ani Muscles
Instrumentation and Techniques for Translabial and Transperineal Pelvic Floor Ultrasound
2D/3D Endovaginal and Endoanal Instrumentation and Techniques
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
