Heller myotomy (partial thickness incision of lower esophageal sphincter)
– Partial (Toupet) fundoplication often incorporated into myotomy procedure
Per-oral endoscopic myotomy (POEM) procedure
– Relief of symptoms with fewer complications
(Left) Upright frontal esophagram shows a dilated esophagus with an abrupt taper (“bird beak”) just above the gastroesophageal (GE) junction . Note the absent gastric air bubble and the fluid-barium level within the esophagus.
(Right) Esophagram shows a grossly dilated, tortuous esophagus with a “sigmoid” appearance. This is an example of longstanding achalasia.
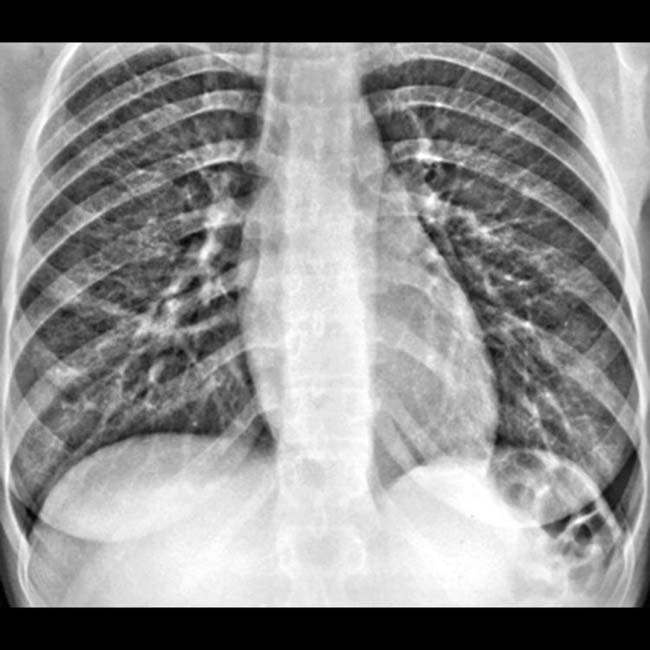
(Left) Upright chest radiograph shows an absent air-fluid level in the stomach of a 28-year-old woman with a recent onset of dysphagia and halitosis.
(Right) Esophagram in the same young woman shows marked dilation of the esophageal lumen ending in a smoothly tapered “bird beak” deformity .
TERMINOLOGY
Synonyms
• Cardiospasm
Definitions
• Primary esophageal motility disorder due to defective neural stimulation of lower esophageal sphincter
IMAGING
General Features
• Best diagnostic clue
“Bird beak” deformity: Dilated esophagus with smooth, symmetric, tapered narrowing at esophagogastric region
• Morphology
Grossly dilated esophagus with smooth tapering at lower end of esophagus
• Other general features
Classified based on etiology
– Primary (idiopathic)
– Secondary (pseudoachalasia)
Manometric characteristics of achalasia
– Absence of primary peristalsis
– Increased or normal resting lower esophageal sphincter (LES) pressures
– Incomplete or absent LES relaxation on swallowing
Variants of achalasia: Atypical manometric findings
– Early: Characterized by aperistalsis with normal LES pressure
– Vigorous: Simultaneous high amplitude and repetitive contractions
– Both variants are transitional and finally evolve into classic achalasia
 Transient flow of fluid into stomach when hydrostatic pressure of fluid column exceeds tonic LES pressure
Transient flow of fluid into stomach when hydrostatic pressure of fluid column exceeds tonic LES pressure









 . Note the absent gastric air bubble and the fluid-barium level
. Note the absent gastric air bubble and the fluid-barium level  within the esophagus.
within the esophagus.

 .
.











 Primary achalasia
Primary achalasia Secondary achalasia (pseudoachalasia)
Secondary achalasia (pseudoachalasia)




