• CREST syndrome: Minimal cutaneous and late visceral
C: Calcinosis of skin
R: Raynaud phenomenon
E: Esophageal dysmotility
S: Sclerodactyly (involvement of fingers)
T: Telangiectasia
• Esophagography
Atony or aperistalsis: Lower 2/3 (smooth muscle)
Mild to moderate dilatation of esophagus
Patulous lower esophageal sphincter (early)
Ulcers, fusiform peptic stricture (later)
Gastroesophageal reflux (70% of patients)
40% develop Barrett esophagus
TOP DIFFERENTIAL DIAGNOSES
• Esophageal achalasia
• Reflux esophagitis (with stricture)
• Esophageal carcinoma
• Iatrogenic
(Left) Upright film from an esophagram in a 29-year-old woman with dysphagia and shortness of breath shows a dilated, atonic esophagus with a distal esophageal stricture . Esophageal peristalsis was completely absent.
(Right) Chest CT in the same patient shows interstitial fibrosis and a massive dilated esophagus , all findings due to scleroderma.
(Left) Film from an esophagram in a young woman with dysphagia shows a dilated esophagus with a persistent air-fluid level, indicating delayed emptying. There is stricture of the distal esophagus .
(Right) Subsequent film in the same patient shows a dilated duodenum with functional narrowing of its 3rd portion. The duodenum is often dilated and atonic in patients with scleroderma.
TERMINOLOGY
Synonyms
• Progressive systemic sclerosis
Definitions
• Multisystem disorder of small vessels and connective tissue (collagen vascular disease) of unknown etiology
IMAGING
General Features
• Best diagnostic clue
Dilated atonic esophagus with distal stricture (late findings)
• Other general features
Multisystemic disorder with immunologic and inflammatory changes
Characterized by atrophy, fibrosis, and sclerosis of skin, vessels, and organs
Involves skin, synovium, and parenchyma of multiple organs
– Gastrointestinal tract, lungs, heart, kidneys, and nervous system
Gastrointestinal (GI) tract scleroderma
– 3rd most common manifestation after skin changes and Raynaud phenomenon
– Seen in up to 90% of patients
– Most common sites: Esophagus > duodenum > anus/rectum > small bowel > colon
– Most frequent cause of chronic intestinal pseudo-obstruction
Scleroderma is classified into 2 types
– Diffuse scleroderma
– CREST syndrome (more benign course)
Diffuse scleroderma: Cutaneous and visceral involvement
– Interstitial pulmonary fibrosis, often severe
– Organ failure more likely
– Associated with antitopoisomerase 1 antibody (anti-Scl 70)
CREST syndrome: Minimal cutaneous and late visceral involvement
– C: Calcinosis of skin
– R: Raynaud phenomenon
– E: Esophageal dysmotility
– S: Sclerodactyly (involvement of fingers)
– T: Telangiectasia
– Associated with anticentromere antibodies
Radiographic Findings
• Fluoroscopic-guided esophagography
Normal peristalsis above aortic arch (striated muscle)
















 with a distal esophageal stricture
with a distal esophageal stricture  . Esophageal peristalsis was completely absent.
. Esophageal peristalsis was completely absent.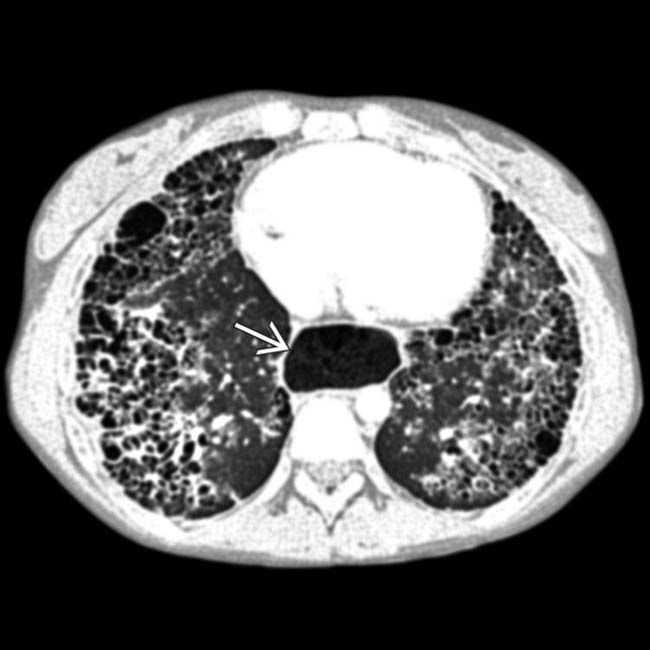
 , all findings due to scleroderma.
, all findings due to scleroderma.
 .
.





















