Fig. 15.1
(a) Diagram of the deep veins in the previously used scheme of the superficial leg veins with great saphenous vein and small saphenous vein (**). (b) Development over time of flow in the great saphenous vein (VSM) with an occluded femoral vein (formerly superficial). Dark red, vertical obstruction; orange dotted line, beginning of muscular systole (toes raised); yellow dotted line, beginning of muscular diastole (toes lowered). The blood flows from the distal calf through a paratibial perforating vein (formerly Boyd; green). The flow is antegrade at first into the great saphenous vein causing its dilatation (violet). (c) Commencement of oscillating volume flow as valve closure starts to fail in the over-dilated great saphenous vein. Furthermore, a deep to superficial drainage flow develops within this segment of refluxive great saphenous vein. This drainage during calf systole can occur either via an incompetent great saphenous vein or an incompetent venous tributary. (d) Refluxive venous tributaries are seen receiving flow volumes from the great saphenous vein. Although the vein is technically refluxive, the considerably large volume of blood with antegrade flow is remarkable. Meanwhile, several refluxive venous tributaries have formed, and the lower part of the great saphenous vein has yielded and become refluxive. This reflux volume fills the deep system at the ankle during muscular diastole. As a result of this increased flow and pressure, the perforating vein dilates and an outward flow may also be recorded in the perforating vein during calf systole
Copyright: [Author]
The flow of blood leaves the deep vein system through a perforating vein. The blood flow in this vein is retrograde, refluxive and outwards. It brings blood from deep to superficial veins (Fig. 15.2) and serves to drain the lower segments of the deep veins because they no longer have a drainage route due to higher obstruction.
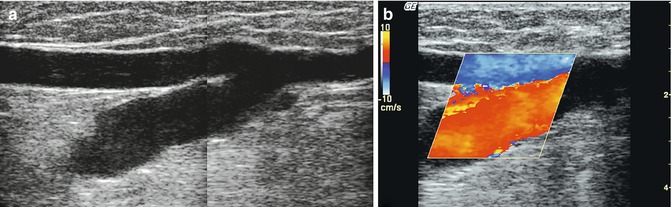
Fig. 15.2
The aftermath of occlusion of the common femoral vein in the right leg due to an abscess in an iv heroin abuser. Dilated perforating veins are seen in the adductor canal (formerly Dodd). These carry blood outwards into the great saphenous vein. This increase in flow causes saphenous dilatation in an attempt to bypass the femoral occlusion. Although most of the blood in the upper part flows antegrade, the lower segment also becomes refluxive which can give rise to several refluxive venous tributaries. (a) Longitudinal view of the inner thigh. Dilated perforating vein in the adductor canal (formerly Dodd) which drains into the great saphenous vein. Right, in the picture, refluxive lower segment of great saphenous vein; left, dilated great saphenous vein with antegrade flow. (b) The same leg in colour duplex during calf-muscle systole. Outward flow is seen in the perforating vein with antegrade flow up to the great saphenous vein. See accompanying online material
Copyright: [Author]
Blood will flow upwards in the superficial veins and then re-enter the deep veins above the point of closure. This occurs usually after femoral vein (formerly superficial) occlusion through the saphenofemoral junction. This pathway is called an open compensatory (vicarious) shunt (Franceschi and Zamboni 2010).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


