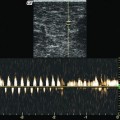
Fig. 8.1
Junction of the small saphenous vein (SSV) in the popliteal fossa with no reflux. (a) Longitudinal view through the popliteal fossa demonstrating the small saphenous vein curving inwards into the popliteal vein, which is also curved. The probe is tilted showing flow away from the probe (left, blue) and towards the probe (right, red). On the right, a muscular vein is seen draining into the tibiofibular trunk. Fasciae are shown in yellow: The muscle fascia follows the gastrocnemius heads (yellow lines) to form the base of the popliteal depression which is completely overarched by the saphenous fascia (orange line) (online material). (b) Transverse view through the popliteal fossa during muscular systole demonstrating antegrade flow in healthy veins (blue)
Copyright: [Author]
In 65 % of legs, the small saphenous vein has a cranial extension. If this vein joins the great saphenous vein, it is called either the Giacomini anastomosis or the femoropopliteal vein. The physiological flow in the cranial extension of the small saphenous vein is towards the small saphenous vein, which is downwards (Fig. 8.2 and Sect. 2.5.3). Alternatively, the proximal extension of the small saphenous vein may terminate directly into a perforating vein on the back of the thigh.
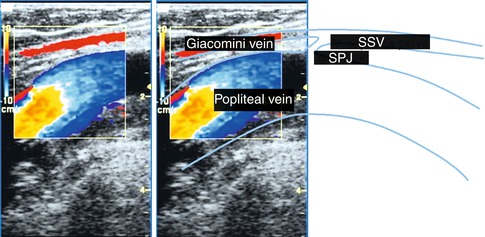
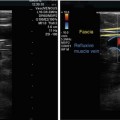
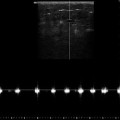
Fig. 8.2
Longitudinal view through the upper part of the popliteal fossa demonstrating the proximal extension of the small saphenous vein or Giacomini vein (online material). Note the physiological downward flow (red) in the Giacomini vein which drains into the small saphenous vein. High-velocity aliasing artefacts are seen in the popliteal vein (yellow and orange)
Copyright: [Author]
Superficial veins along their course are best seen in transverse view. Junctions are demonstrated better in longitudinal view.
8.3.2 Refluxive Anatomy and Flow
If the small saphenous vein is incompetent, it may divert to a greater or lesser degree from the normal locations described. This usually depends upon the lateral spaces which are devoid of investing saphenous fascia and the reflux volume (Fig. 8.3a, b). In cases where the reflux has existed for a long time, it is no longer possible to show the vein in a single image. This is because it becomes very tortuous (Fig. 8.3c, d). This pathological feature is not typical of the great saphenous vein. The explanation may be the fact that the small saphenous vein in the popliteal fossa is not held in a straight course by its fascia. The distance between the popliteal vein and the beginning of the fascial sheath of the small saphenous vein is significantly greater than the corresponding distance in the great saphenous vein. This may be the reason why the great saphenous vein never becomes tortuous at its termination. However, a very dilated termination may still occur.
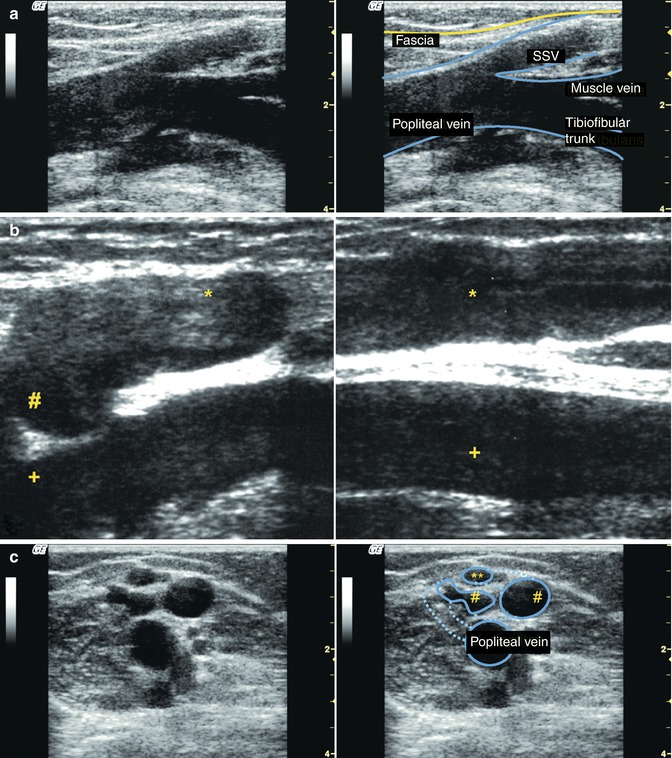
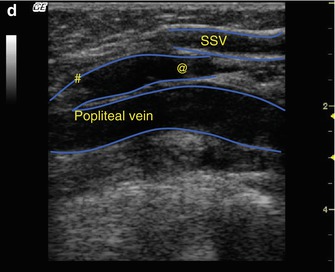
Fig. 8.3
Refluxive small saphenous vein (SSV) at a typical junction with the popliteal vein. (a) With early incompetence, the calibre of the small saphenous vein appears large. The anatomy is almost like a normal finding without reflux (online material). (b) Longitudinal view through the popliteal fossa and proximal calf demonstrating a grossly dilated small saphenous vein at its junction (#) with the popliteal vein (+) (online material). (c) Transverse view through the popliteal fossa with long-standing incompetence of the small saphenous vein. The junction is hard to visualise and the termination is very tortuous occupying several layers (online material). Just below the fascia is the non-refluxive vein of Giacomini (**) immediately before its junction with the small saphenous vein (not shown). The tortuous termination (#) is cut twice in this image. The dotted line reconstructs the terminal course of the vein. (d) Longitudinal view through the same popliteal fossa. The termination of the small saphenous vein appears in the image as a lengthwise vein (#) rather than an inward curve. This can be distinguished from a muscular vein because it cannot be traced further down (@) due to its tortuosity. It eventually meets the straight part of the small saphenous vein
Copyright: [Author]
On rare occasions, an aneurysm may form at the termination of the small saphenous vein which may contain a thrombus (Figs. 8.4 and 8.5).
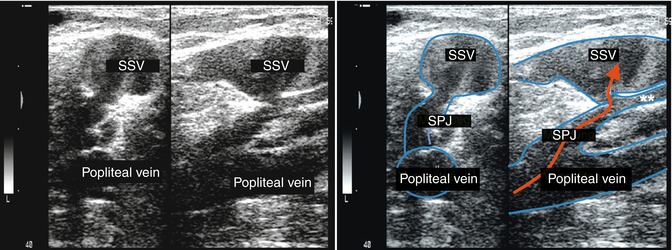
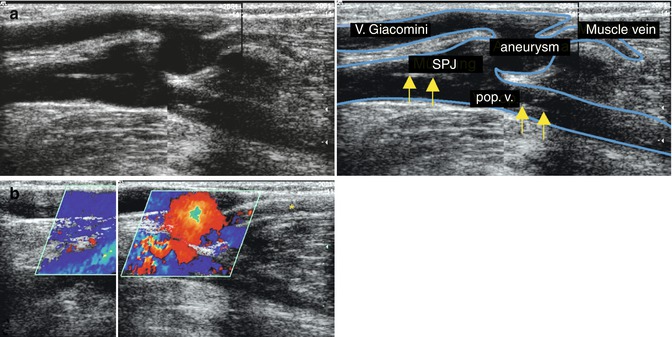
Fig. 8.4
Left transverse, right longitudinal view through the popliteal fossa demonstrating a venous aneurysm at the termination of the small saphenous vein (SSV). This joins the popliteal vein together with a competent muscle vein (**). The aneurysm has partially thrombosed (Fig. 11.5b). The arrow indicates the direction of flow of the refluxive blood
Copyright: [Author]
Fig. 8.5
(a) Longitudinal view through the popliteal fossa demonstrating the aftermath of a femoropopliteal vein thrombosis. Septal formation is apparent in the deep veins (arrowed) which is refluxive (b). The Giacomini vein is dilated and refluxive at its junction with the small saphenous vein. The muscular vein is competent (online material). (b) The same leg as in a with colour duplex ultrasound during muscular diastole. There is an antegrade upward flow (blue, away from probe) in the vein of Giacomini (reflux), which is filled through the incompetent saphenopopliteal junction (red, towards probe). In the right half of the image, the probe was positioned further lateral to demonstrate the small saphenous vein
Copyright: [Author]
8.3.3 Level of Termination of the Small Saphenous Vein
If the small saphenous vein is followed up from the middle of the calf, in very rare cases (<1 %; Sect. 2.5.1), a junction is found with muscle veins or a communicating vein to the great saphenous vein (Fig. 8.6). In this case, the small saphenous vein is no longer visible within its fascia at the proximal calf and the saphenopopliteal junction is absent.
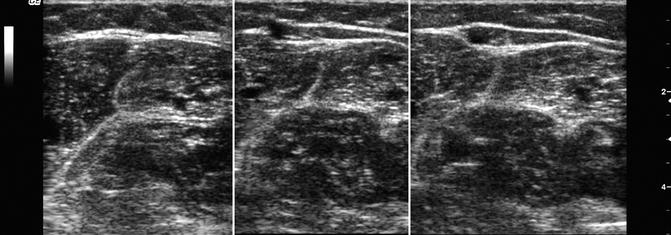
Fig. 8.6
Transverse view through the back of the calf demonstrating agenesis of the small saphenous vein junction. In the upper third of the calf, flow from the small saphenous vein passes through a communicating vein to the great saphenous vein. Left (upper calf) shows the empty fascial compartment. Middle (lower part of upper calf) shows the vein piercing the fascia. Right (mid calf) shows the typical small saphenous vein enclosed in its fascial layers (online material)
Copyright: [Author]
According to Caggiati, 54 % of small saphenous veins join the popliteal vein above the posterior skin crease, and 38 % are higher still at or above the apex of the popliteal fossa (Sect. 2.5.1). It is important to identify preoperatively those cases in which the junction lies under the distal thigh musculature, since dissection with local anaesthesia is much more difficult (Figs. 8.7 and 2.31d). The small saphenous vein does not pierce the muscle. Instead it runs upwards under the musculature for a variable distance. The small saphenous vein seldom joins the popliteal vein directly from a posterior route (Fig. 8.3a). More often it joins the deep vein from lateral or medial (Fig. 8.7a, b). When there is a high junction, the tibial and peroneal nerves run close to the veins (Sect. 17.6). It is essential to scan the patient just prior to surgery in order to assess the expected anatomy. This information can make the vein easier to find and identify during dissection.
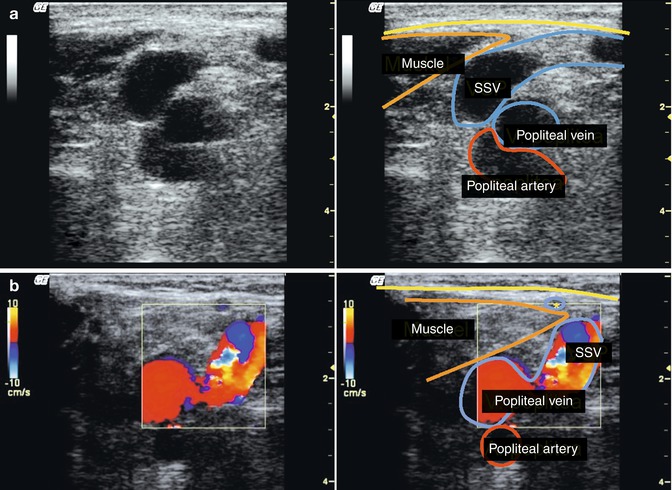
Fig. 8.7
(a) Transverse view 7 cm above the left popliteal skin crease demonstrating a high junction of the small saphenous vein (SSV). This is at the apex of the popliteal fossa where the vein is seen running underneath the thigh musculature to join the popliteal vein from a lateral approach (online material). (b) Transverse view through the distal thigh of the left leg with the small saphenous vein joining the popliteal vein from the medial side (* vein of Giacomini)
Copyright: [Author]
When the junction is above the apex of the popliteal fossa, a large incision is required to expose the deep leg vein prior to ligation. The importance of a preoperative ultrasound scan cannot be overestimated for planning the surgical strategy. This should complement the ultrasound scan report performed at the time of diagnosis. In these cases, the junction lies very deep under the thigh musculature (Fig. 8.8
 Examination of Superficial Veins in the Presence of Deep Venous Disease
Examination of Superficial Veins in the Presence of Deep Venous Disease
 Duplex Ultrasound Examination of Superficial Leg Veins
Duplex Ultrasound Examination of Superficial Leg Veins
 Flow Provocation Manoeuvres for the Diagnosis of Venous Disease Using Duplex Ultrasound
Flow Provocation Manoeuvres for the Diagnosis of Venous Disease Using Duplex Ultrasound
 The Ultrasound Scanner
The Ultrasound Scanner
 Examination of the Great Saphenous Vein
Examination of the Great Saphenous Vein
 Anatomy of the Superficial Veins
Anatomy of the Superficial Veins




Related posts:
Examination of Superficial Veins in the Presence of Deep Venous Disease
Duplex Ultrasound Examination of Superficial Leg Veins
Flow Provocation Manoeuvres for the Diagnosis of Venous Disease Using Duplex Ultrasound
The Ultrasound Scanner
Examination of the Great Saphenous Vein
Anatomy of the Superficial Veins
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
