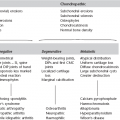
11 11.1 Orbital mass lesions 1. Retinoblastoma – usually presents with white pupil; 20–40% bilateral, 10% have family history; four main subgroups: (c) Chromosomal – associated with partial deletion of chromosome 13. (d) ‘Trilateral’ retinoblastoma – bilateral retinoblastoma with pineal tumour. 90% show (various patterns of) calcification. 2. Melanoma – increased incidence from middle age; avidly enhances; may be high signal on precontrast T1 if melanotic. 2. Thyroid eye disease – enlargement of muscles; swelling of intraorbital fat. 3. Rhabdomyosarcoma – 10% arise in orbit, 50% < 7 years of age; rapid-onset proptosis with deviation of globe; although arises in muscle most of tumour usually extraconal; differentiation between orbital and extraorbital (parameningeal) origin important as treatment differs. 1. Orbital cellulitis and abscess – coronal sections with contrast most sensitive, especially for small subperiosteal collections; secondary to paranasal sinus infection. 4. Dermoid – commonest at external angle. 5. Lymphangioma/lymphaemangioma. 6. Direct extension of lacrimal gland tumour. 7. Langerhans’ cell histiocytosis. 8. Direct extension of paranasal sinus tumour. 11.2 Optic nerve glioma versus optic nerve sheath meningioma – clinical and radiological differentiation 11.5 Enlarged optic foramen Normal range = 4.4–6 mm; ≥ 7 mm, or greater than 1 mm difference with asymptomatic side = abnormal.
Face and neck
Lesions involving the globe
Intraconal lesions
Conal lesions
Extraconal lesions
Glioma
Meningioma
50% < 5 years of age
Usually middle-aged women
± Bilateral
Usually unilateral
Slowly progressive, painless loss of vision; central scotoma
Childhood tumours may remain quiescent for years, particularly in the presence of NF
Adult tumours more aggressive
Slowly progressive, painless loss of vision; proptosis
Neurofibromatosis*: NF-1 in 25%; 15% of NF-1 have optic nerve glioma; bilateral disease strongly suggests neurofibromatosis
Neurofibromatosis (1 or 2) in 4–6%; bilateral disease may occur with or without NF
No orbital hyperostosis
Hyperostosis
Widened optic canal in 90% but intracranial extension is unusual
Widened optical canal in 10%
Kinking and buckling of the optic nerve is common. Smooth outline
Straight optic nerve, but tumour may be eccentric
Well-defined margins
More infiltrative
Localized or fusiform thickening
Calcification rare without prior radiotherapy
Calcification (linear, plaque-like or granular) more common
Isointense to brain on T1W MRI; hyperintense on T2W MRI
Similar signal to optic nerve on most unenhanced MR pulse sequences
Variable contrast enhancement with mottled lucencies due to mucinous degeneration
Diffuse homogeneous enhancement ± serrated margins
Negative image of optic nerve within the tumour (tram-track sign)
Face and neck