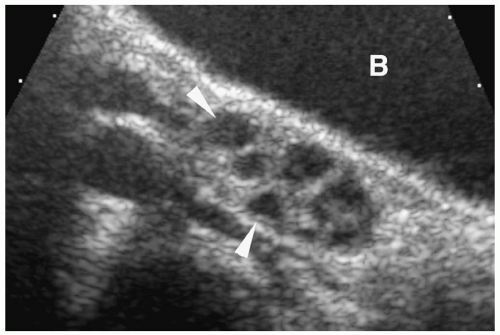
 Figure 10.1 Normal prepubertal ovary. Longitudinal sonogram of the right ovary of a 2-year-old girl shows multiple small follicles (arrowheads), measuring less than 9 mm in diameter (B, bladder). |
Table 10.1: Ovarian Volume Measurements | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
stimulated follicle can attain a size of 20 to 30 cm, before it ruptures and releases its ovum. The ruptured follicle involutes and becomes a corpus luteum, unless the ovum is fertilized. Corpus luteum follicles range between 10 and 30 mm in diameter. Of note, the diameter of a physiologic cyst should be 3 cm or less.
 Figure 10.2 Normal pubertal ovary. A. Estrogen phase. Longitudinal sonogram on day 10 of the menstrual cycle shows multiple follicles less than 10 mm in diameter (arrowheads). B. Progesterone phase. Longitudinal sonogram on day 20 of the menstrual cycle shows a dominant cyst (arrow), measuring 18 mm in length. This likely represents a corpus luteum cyst. |
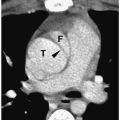
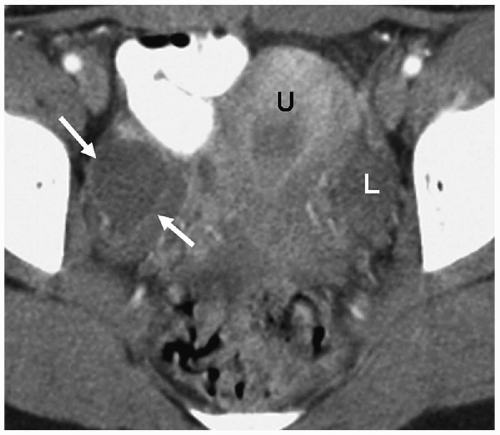 Figure 10.3 Normal pubertal ovaries. CT scan of a 15-year-old girl on day 12 of the menstrual cycle demonstrates a stimulated follicle (arrows) measuring 25 mm in diameter in the right ovary. A normal low attenuation left ovary (L) is seen. (U, uterus). |
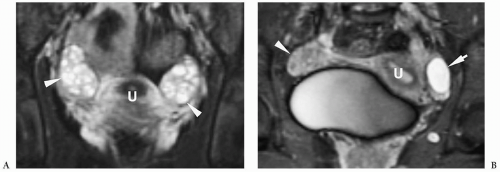 Figure 10.4 Normal pubertal female pelvis, MRI. A. Coronal T2-weighted fat-saturated MR image of a 14-year-old girl demonstrates multiple bright follicles in the cortex of the ovaries (arrowheads). Some normal intermediate signal stromal tissue also can be noted (U, uterus). B. T2-weighted MR of another adolescent girl on day 10 of the menstrual cycle shows a high-intensity cyst, measuring 20 mm in diameter, in the left ovary (arrow), representing a developing follicle (U, uterus; arrowhead, right ovary). |
Table 10.2: Normal Uterine Diameters and Volume | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
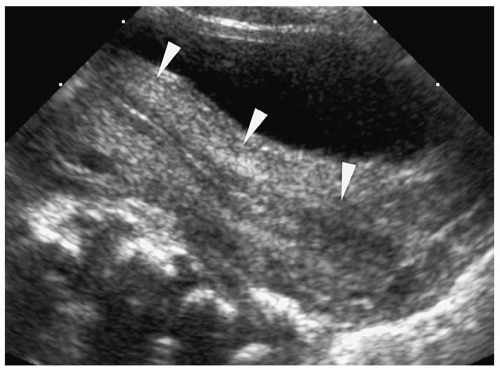 Figure 10.5 Normal neonatal uterus, sonogram. Longitudinal sonogram shows prominence of the uterine fundus (arrowheads) and a thin, hyperechoic endometrial stripe, as a result of in utero hormonal stimulation. |
myometrium and endometrium cannot be differentiated from each other (Fig. 10.9). Three distinct zones can be seen within the fundus on T2-weighted MR images: the high signal intensity endometrium, low signal intensity inner myometrium, and intermediate signal intensity outer myometrium (Fig. 10.10).
 Figure 10.6 Normal prepubertal uterus, sonogram. Longitudinal sonogram of a 2-year-old girl. The uterus (arrows) is small and tubular with no differentiation between fundus and cervix. Zonal anatomy is indiscernible. There is no recognizable endometrial stripe. |
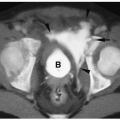
 Figure 10.7 Normal prepubertal uterus, CT. CT scan of a 5-year-old girl. The uterus (arrow) appears as a small homogeneous, oval soft-tissue structure posterior to the bladder. Neither ovary is visualized. |
of the female reproductive tract, the lower segments of the paired müllerian ducts fuse to form the uterus, cervix, and upper vagina. After the lower müllerian ducts fuse, a central septum is present, which eventually resorbs to form a single uterine cavity and cervix. Uterine anomies result when there is an error in development or fusion of the ducts or resorption of the midline septum. Patients may present with primary amenorrhea, mass (hematocolpos), or delayed onset of menarche. Coexistent renal ectopia or agenesis occurs in 20% to 30% of patients. Ultrasonography and MRI are the studies of choice to detect and characterize müllerian duct anomalies (11,12). The most common anomalies are discussed below.
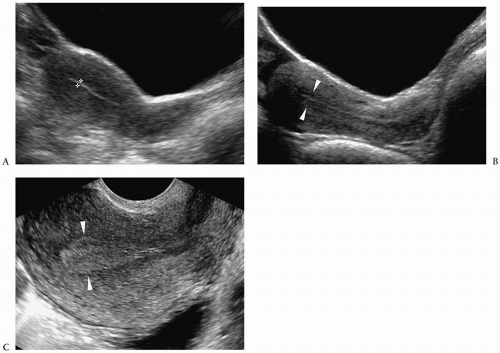 Figure 10.8 Normal pubertal uterus. Three different patients. A. Early menstrual phase. Longitudinal sonogram shows a 3-mm thick echogenic endometrial stripe (cursors). B. Proliferative phase. Longitudinal sonogram near the time of ovulation shows an 8-mm-thick endometrial stripe (arrowheads). C. Secretory phase. Longitudinal sonogram shows an endometrial stripe thickness of 15 mm (arrowheads). Note in all three patients that there is pear-shaped uterus, with a fundus that is larger than the cervix. |
 Figure 10.9 Normal pubertal uterus. Contrast-enhanced CT scans of a 15-year-old girl shows a low-attenuation right ovary (R) and the uterine fundus (arrow). The higher attenuation myometrium and endometrium can be differentiated from the lower attenuation endometrial canal, but they cannot be differentiated from each other. |
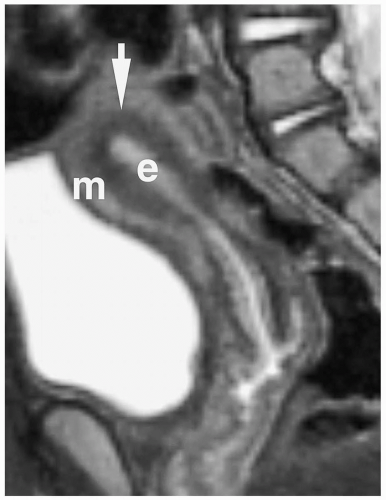 Figure 10.10 Normal pubertal uterus. Zonal anatomy is well seen on a sagittal T2-weighted image from a 12-year-old girl. The high-intensity endometrial complex (e) is surrounded by the low-intensity signal of the junctional zone (arrow) and the outer intermediate signal intensity myometrium (m). |
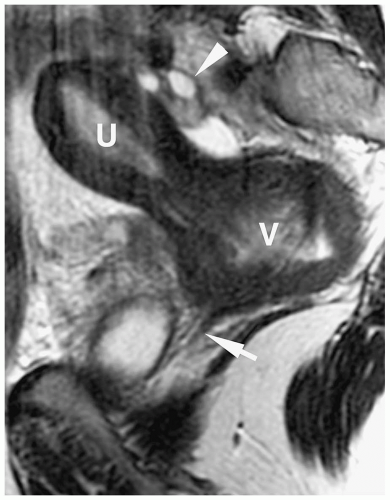 Figure 10.11 Mayer-Rokitansky-Kuster-Hauser syndrome (uterine hypoplasia), 15-year-old girl with amenorrhea. Sagittal T2-weighted image shows a small uterus with fluid within the uterine canal (U) and upper one-third of the vagina (V). There was atresia of the lower two-thirds of the vagina (arrow) documented at surgery. Note the poor zonal definition of the uterus, and a normal ovary (arrowhead). |
banana-shaped uterus (fusiform uterine cavity with lateral deviation) with normal zonal anatomy. Partial arrest in development of one duct results in a rudimentary uterine horn, which may or may not connect to the opposite cornua (Fig. 10.12). If the rudimentary horn is obstructed and contains functioning endometrium, it may be distended by blood or blood products. Unicornuate uterus does not require treatment unless there is hematometra.
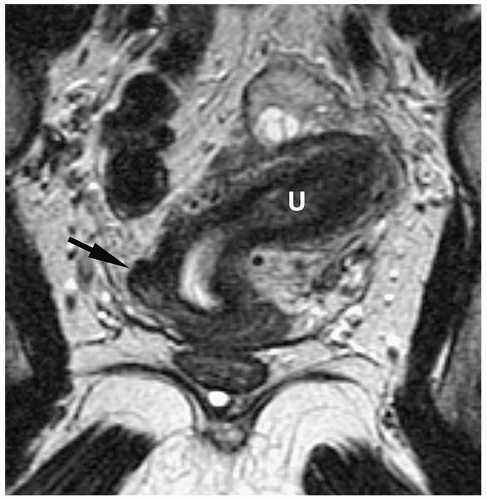 Figure 10.12 Unicornuate uterus with a noncommunicating rudimentary horn. A coronal T2-weighted image shows a hypoplastic right uterine horn (arrow), which does not communicate with the normal left uterine horn (U). The left uterine horn is deviated laterally and has differentiated zonal anatomy. |
 Figure 10.13 Müllerian duct fusion anomalies. A. Uterus didelphys: two uteri, two cervices, two vaginas. B. Uterus duplex bicollis: two uteri, two cervices, one vagina. C. Uterus duplex unicollis (bicornuate uterus): two uteri, one cervix, one vagina. D. Uterus septus: a single uterus divided by a septum. (Adapted from Colodny AH. Disorders of the female genitalia. In: Kelalis PP, King LR, Belman AB, eds. Clinical pediatric urology. Philadelphia: W.B. Saunders, 1985;888-903.) |
bicornuate uterus from septate uterus is the fundal contour. Differentiation is important because septate uteri are treated with transvaginal hysteroscopic resection of the septum, while an abdominal approach is required for the bicornuate uterus.
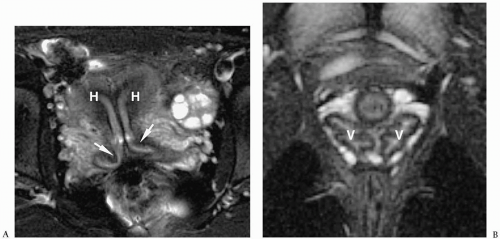 Figure 10.14 Uterus didelphys. A. Oblique coronal T2-weighted fat-saturated MR image demonstrates two uterine horns (H) and two cervices (arrows). B. Axial fast spin-echo (FSE) T2-weighted fat-saturated image shows two vaginas (V). |
 Figure 10.15 Bicornuate uterus. Fat-saturated T2-weighted MR image shows two uterine bodies (arrows). There is a deep cleft (> 1 cm) in the uterine fundus. Each uterine horn is of similar size and has differentiated zonal anatomy. The two bodies fused just above a single cervix.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|