Fig. 12.1
Anatomic diagram of the developmental stages from ovarian follicle to luteal body. Counterclockwise from left: primordial and primary follicles, maturing follicles, ruptured follicle (or hemorrhagic body), luteal bodies, initial and mature, corpus albicans (arrowhead). The arrow indicates a released egg
Located on the posterior surface of the broad ligament and the lateral wall of the lesser pelvis, the ovary occupies the “ovarian fossa,” bounded on the rear side by the ureter and the iliac vessels. The ovaries show an upper or tubal pole, an inferior or uterine pole, the hilum border to which the mesovarium is attached, and a posterior free border. The ovarian ligament originates from the uterine pole and is inserted in the body of the uterus posterior to the intramural portion of the uterine tube. Laterally, the suspensory ligament anchors the ovary to the pelvic wall and conveys the vessels, nerves, and efferent and afferent lymphatic vessels. The ovary is also anchored by the mesovarium, a short peritoneal ligament which detaches from the broad ligament and the tubo-ovarian ligament connecting the upper pole of the ovary to the infundibulum of the uterine tube (Fig. 12.2).
Fig. 12.2
Anatomical diagram of the female reproductive system. Uterus (1), tubal isthmus (2), ampulla (3), infundibulum (4), suspensory ligament of the ovary (5), mesovarium or mesosalpinx (6), ovary (7), ovarian ligament (8), broad ligament (9), and ureter (10). The arrow indicates a luteal body
The main blood supply is provided by the ovarian artery (branch of the aorta) contained in the suspensory ligament. A second source is provided by the ovarian branch of the uterine artery, which follows the uterine ligament and sends branches through the mesovarium which anastomose with those of the ovarian artery. The venous network forms the pampiniform plexus at the level of the ovarian hilum: the veins arising from the plexus merge together forming the ovarian vein, which initially runs inside the suspensory ligament and then empties into the renal vein on the left and the inferior vena cava on the right.
The lymphatic vessels of the ovaries are abundant and drain into the preaortic and para-aortic lymph nodes.
Innervation of the ovary is provided by the nerve branches that, along with the arteries, form the ovarian plexus, an extension of the celiac and renal plexuses.
12.1.2 Uterine Tubes or Oviducts
Together with the ovaries, the fallopian tubes or oviducts may be considered as annexes of the uterus. They are a pair of symmetrical muscular-membranous conduits which create a communication between the uterine and peritoneal cavities; they are essential for capturing the cells after ovulation and their transport toward the uterus, for the migration of spermatozoa, and their capacitation, for the fertilization and conveying the embryo toward the uterus as well as for the early phases of its development.
Each tube is located in the superior wing of the broad ligament, lateral to the uterus, anterior to the ovary, and posterior to the round ligament; they originate from the uterine horns, running obliquely toward the top, laterally and posteriorly toward the pelvic sidewall; nevertheless the position is very variable, sometimes it lies in the ovarian fossa and some other times in the rectouterine pouch.
The average length is 12–18 cm; the lumen diameter varies from 0.5 to 1 mm, at the insertion on the uterus, up to approximately 8–15 mm at the distal end of the ampulla.
Anchorage of the uterine tube is provided by continuity with the uterus and tubo-ovarian ligament which connects the distal portion of the tube to the upper pole of the ovary.
Each uterine tube is divided into four parts, located in a medial-lateral direction:
The intramural segment with a length of 1–2.5 cm, which passes through the myometrium and communicates with the uterine cavity by the opening of the uterine tube
The isthmus (2–3 cm), an almost straight segment which follows the uterine horn
The ampulla (length 6–8 cm), a segment with alternating dilatations and constrictions in the lumen
The funnel-shaped infundibulum (1–2 cm), which ends into fringed extensions, called fimbriae, to delimit an opening forming the communication between the tubal lumen and the peritoneal cavity (abdominal ostium of the uterine tube) (Fig. 12.2)
The arterial vascularization of the uterine tubes is supplied by the arterial arches formed by the anastomosis of the uterine and ovarian arteries. The venous outflow takes place in the uterine and ovarian veins.
12.1.3 Uterus
The uterus is a hollow, unpaired, and median muscular organ, located in the pelvic cavity posterior to the urinary bladder and anterior to the rectum. It is conical in shape with the base upward and the trunk, forming the apex, oriented downward.
At birth the uterus is relatively large and has a configuration similar to the adult one, since during pregnancy it experiences the hormonal stimulation of the maternal estrogens. In a later moment the uterus decreases in size (2–3 cm in length and 0.5–1 cm in width), keeping it until puberty when it grows volumetrically and shows a pyriform shape, while in menopause it undergoes a progressive atrophy. The average dimensions in a nulliparous woman are 6.5 cm in length, 4 cm in width, and 2 cm in thickness; the measurements and weight of the uterus are slightly greater in women with prior pregnancies. The capacity of the uterine cavity is about 4 mL in nulliparous and 5–6 mL in pluriparous woman.
The uterus can be divided into three parts, anatomically and functionally separated: the body, the isthmus, and the neck (or cervix). The body is the upper part of the organ and has a flat or slightly convex anteroinferior surface, a convex posterosuperior surface, and rounded lateral borders. The highly convex upper border corresponds to the part of the uterus that projects beyond a plane through the entrance point of the uterine tubes and is called the fundus. The isthmus is a slight constriction between the body and the cervix and has an anatomical-functional role during labor only. The cervix represents the inferior part of the uterus where the vagina is inserted. In relation to the insertion point, we can distinguish a supravaginal and a rounded vaginal portion (“portio vaginalis”), whose distal end communicates with the vagina via the external uterine os.
The uterine cavity is flattened from the front to the back and is divided into two parts by the isthmus: the cavity of the body, triangular in shape and virtual, and the cavity of the cervix, spindle shaped and real (Fig. 12.3).
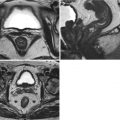
Fig. 12.3
Anatomical diagram of the uterus. Coronal section. Fornix vaginalis (1), external uterine os (2), cervical canal (3), internal uterine os (4), isthmus (5), body (6) and fundus (7) of the uterus, intramural segment of the uterine tube (8), and ovary (9)
While it is normally located in an anteverted and anteflexed position, the uterus may sometimes be found in an anomalous position (retroversion, lateroversion, etc.), due to congenital or acquired causes, generally inflammatory in nature. Indeed its axis forms an angle of 90° (version angle) with the angle of the vagina; the axis of the cervix forms an opened angle of 100–120° with the axis of the body (flexion angle). This position is maintained by a complex system of connections which is schematically composed of support, backing, and directional structures. The main supports are the connective muscular structures of the pelvic floor. The suspensory structures consist of the uterosacral ligaments (posteriorly), the vesicouterine ligament (anteriorly), and the cardinal, transverse cervical, ligaments (laterally); the latter are formed by a thickening of the subperitoneal connective tissue and run at the base of the broad ligaments, forming a robust transverse band of tissue which connects the supravaginal cervix and the vagina to the lateral wall of the pelvis. The directional system has the function of keeping the uterine anteversion (round ligaments, two muscular fiber cords accompanied by vessels extending from the uterine tubes to the labia majora and the pubis passing through the inguinal canal) and limiting the lateroversion (broad ligaments, consisting of a double layer of peritoneum which connects both sides of the uterine body to the lateral wall of the pelvis).
The uterus is a subperitoneal organ. The parietal peritoneum, in fact, descends from the anterior wall of the abdomen; is reflected onto the urinary bladder, partially covering it; and returns to the anterior wall of the uterus. After covering the uterine fundus, the serous peritoneum descends over the posterior surface of the uterus, also covering a part of the posterior vaginal wall, and is reflected again to cover the rectum, thus forming the rectouterine pouch or pouch of Douglas (Fig. 12.4). Laterally, the anterior and posterior parietal peritoneum layers join to form the broad ligaments.
Fig. 12.4
Sagittal anatomic diagram of the pelvis in a female subject. Bladder (1), uterine body (2), cervix (3), rectouterine pouch (4), rectum (5), rectovaginal septum (6), and vesicovaginal septum (7)
The blood supply of the uterus derives chiefly from three arteries: the uterine artery, the ovarian arteries, and the artery of the round ligament.
The uterine wall structurally consists of three layers from the inner to the outer side: the mucous (endometrium), muscular (myometrium), and serous (perimetrium) layers.
12.1.4 Vagina
The vagina is a median muscular-membranous conduit around 8 cm in length which extends from the uterus to the vulva. Running obliquely downward and forward, it is located partly in the pelvis and partly in the perineum. The superior end surrounds the uterine cervix between the inferior third and the middle, thus forming a recess called the vaginal fornix which is usually described as having four segments: anterior, posterior, right lateral, and left lateral.
The anterior wall of the vagina is related to the urinary bladder from which it is separated by relatively loose connective tissue, the vesicovaginal septum, and to the urethra via a dense fibrous urethrovaginal septum. The posterior wall, at the level of the fornix, is related to the rectouterine pouch, while caudally it is closely related to the rectum from which it is separated by the rectovaginal fascia. The lateral walls of the pelvic segment above the levator ani muscle correspond to the base of the broad ligament.
The vagina is supplied on each side, from top to bottom, by branches of the uterine artery, the vaginal artery (branch of the iliac), and the middle rectal artery.
The external and internal iliac and hypogastric lymph nodes drain the lymphatic vessels of the upper part of the vagina; the more internal iliac lymph nodes and the lymph node of the Gerota drain the middle part (between the vagina and the rectum), while the superficial inguinal lymph nodes drain the inferior part.
12.1.5 Vulva
The vulva is made up of the female external genitalia. Bounded by the medial aspects of the thighs, the vulva extends anteroposteriorly immediately below the pubic symphysis up to around 3 cm, in front of the anus. It includes the mons pubis, labial majora, labia minora, vestibule, clitoris, and greater vestibular glands (the vestibular Bartholin’s glands and the periurethral Skene’s glands).
The arterial vascularization consists of the external, superior, and inferior pudendal arteries (branches of the femoral) and the internal pudendal artery (branch of the internal iliac).
The lymph nodes which drain the rich network of the lymphatic vessels of the vulva are the superficial inguinal, deep inguinal (clitoris), and iliac (Bartholin’s glands) lymph nodes.
12.2 Normal Imaging Anatomy
12.2.1 Conventional Radiology
Hysterosonosalpingography is widely used as reference radiologic technique for the evaluation of the female infertility and to assess the patency of the uterine tubes; it also enables the morphologic study of the uterine cavity.
The examination is preferably performed between the 8th and 12th day of the menstrual cycle or at any rate after the cessation of the menstrual flow and before ovulation. In this time window, pregnancy is unlikely. It is generally performed as an outpatient procedure, with no need for any special preparation by the patient, except for a minimal antibiotic coverage.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


