Fig. 6.1
Anatomy of the mediastinum, anterior view. SVC superior vena cava
Fig. 6.2
Anatomy of the mediastinum, sagittal view. H heart, D diaphragm
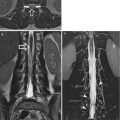
Fig. 6.3
Anatomy of the mediastinum, axial view. IVC inferior vena cava, Ling lingula, LLL left lower pulmonary lobe, LV left ventricle, ML middle pulmonary lobe, RLL right lower pulmonary lobe, RV right ventricle
The mediastinum is superiorly delimited by a plane passing on the superior margin of the first rib, through the superior plate of the first dorsal vertebra, while inferiorly, it is delimited by the diaphragm; laterally, by the parietal layers of the mediastinal pleura; anteriorly, by the internal surface of the sternum; and posteriorly, by the anterior surface of the dorsal vertebrae.
Considerable controversy has ranged over the years concerning the most practical and informative method of dividing the mediastinum into compartments. The subdivision of the mediastinum is not absolute; it rather depends on the different anatomical, radiological or surgery criteria adopted. According to Gray’s Anatomy, the mediastinum is divided into the superior and inferior mediastina; the latter can be further distinguished into the anterior, middle and posterior parts. The inferior and superior mediastina are delimited by a plane passing through the inferior margin of the sternal manubrium and the inferior margin of the fourth dorsal vertebra. The space on the inferior areas of the mediastinum, included between the base of the heart, the diaphragm and the anterior chest wall, is termed cardiophrenic space, mainly occupied by adipose tissue (also the organs and the structures of the different areas of the mediastinum are surrounded by mainly adipose connective tissue).
6.1.1.1 Superior Mediastinum
The superior mediastinum is cranially delimited by a plane passing on the superior margin of the first rib and the superior margin of the first dorsal vertebra, while caudally it is delimited by a plane between the inferior margin of the sternal manubrium and the fourth thoracic vertebra. Anteriorly, it is delimited by the sternal manubrium, posteriorly by the first fourth dorsal vertebrae and laterally by the parietal layer of the mediastinal pleura that covers the apical part of the lungs. The superior mediastinum is therefore a transition area between the cervical and the thoracic regions and includes the origin of the sternohyoid and sternothyroid muscles, the distal part of the long neck muscle, the aortic arch, the innominate artery (or brachiocephalic artery), left common carotid and subclavian arteries, left and right supreme intercostal veins, the superior vena cava, left and right brachiocephalic veins and part of the azygos and hemiazygos veins. We also find some nerve structures, the proximal portion of the vagus nerve, the left recurrent laryngeal nerve and the superior portion of the phrenic and cardiac nerves. The last structures of the superior mediastinum are the trachea, the proximal portion of the oesophagus and the superior part of the thymus and lymph nodes.
6.1.1.2 Inferior Mediastinum
The anterior mediastinum is delimited by the sternum, anteriorly, and, posteriorly, by the anterior surface of the parietal layer of the pericardium and the big mediastinal vessels; laterally, it is delimited by the anterolateral portion of the mediastinal parietal pleurae. It contains lymph vessels and lymph nodes and the internal mammary veins and arteries. In children and teenagers, the thymus occupies most of the anterosuperior part of the mediastinum and a small portion of the anteroinferior one; such an organ has two lobes and its size and activity depend on the age: during puberty it reaches its maximum size and progressively reduces; however, also in adults there is a remaining portion of active parenchyma.
The middle mediastinum is delimited, anteriorly, by the anterior parietal pericardial layer and, posteriorly, by the posterior parietal layer. It includes the heart, pericardium, heart vessels and nerves, common arterial trunk, main pulmonary arteries, bronchial arteries and veins, distal portion of the pulmonary veins, ascending aorta and inferior tract of the aortic arch, superior vena cava and part of the inferior vena cava and azygos veins. Other structures of the middle mediastinum are the carina of the trachea, main bronchi, lymph nodes and lymph vessels and superior phrenic arteries and phrenic nerves.
The posterior mediastinum is delimited by the posterosuperior mediastinal pleura. In the posterior mediastinum we find the descending aorta; the thoracic portion of the oesophagus; posterior intercostal arteries and veins; middle oesophageal arteries and veins; and azygos, hemiazygos and accessory hemiazygos veins. The left and right vagus nerves are, respectively, located in the front and behind the oesophagus; the ganglia of the thoracic sympathetic system are other nerve structures.
The thoracic duct and some other lymph nodes are the most important lymphatic elements. In physiological conditions the lymph nodes of the mediastinum have a diameter between few and of 20 mm (or less); they can increase for infectious or oncologic diseases. Table 6.1 shows the anatomical classification of the mediastinal lymph nodes currently used by the IASLC (International Association for the Study of Lung Cancer).
Table 6.1
Classification of the mediastinal lymph nodes according to the IASLC (J Thorac Oncol 4: 568–577, 2009)
Station site |
|---|
1R and 1L Low cervical, supraclavicular and sternal nodes |
2R and 2L Superior paratracheal nodes |
3a (Prevascular) Prevascular nodes (in front and above the superior vena cava) |
3p (Retrotracheal) Prevertebral nodes |
4R and 4L Lower paratracheal nodes |
5 Subaortic nodes |
6 Paraortic nodes (anterior and lateral to the ascending aorta and aortic arch) |
7L and 7R Subcarinal nodes |
8 Paraoesophageal nodes |
9 Pulmonary ligament nodes |
10 Hilar nodes |
11 Interlobar nodes |
12 Lobar nodes |
13 Segmental nodes |
14 Subsegmental nodes |
On the right of the middle tracheal line |
On the left of the middle tracheal line |
6.1.2 Vascular Mediastinum
In the following paragraph, you will find a description of the most important vascular structures of the mediastinum.
6.1.2.1 Aorta
It is the main artery of the human body, divided in three parts: ascending part, arch and descending part.
The ascending aorta originates at the level of the aortic semilunar valve of the left ventricle; above the origin, there is a physiological dilated structure called aortic bulb where the coronary arteries, supplying the myocardial vascularisation, originate. From a topographical point of view, the ascending aorta is anteriorly related to the conus arteriosus of the right ventricle and the right auricula, superiorly, with the right lung and the residual thymic tissue and, posteriorly, with the left atrium and the right pulmonary artery.
The aortic arch starts at the level of the superior margin of the second right sternocostal articulation; it goes backward and toward the left, in front of the trachea, and passes on its left side; it terminates at the level of the fourth thoracic vertebra. The brachiocephalic arterial trunk (innominate artery), the common carotid artery and the left subclavian arteries are branches of the aortic arch. On the concave margin we find the origin of the ligament connecting the aortic arch with the left pulmonary artery, embryonic rest of the Botallo’s duct. Inferiorly, the aortic arch is connected to the pulmonary trunk bifurcation, anteriorly to the pericardium and posteriorly to the oesophagus and the spinal column.
The descending aorta is divided into the thoracic and abdominal segments, delimited by the passage through the diaphragm, at the level of the twelfth thoracic vertebra. After the origin of the left subclavian artery, the descending aorta is characterised by a narrowing called aortic isthmus; then, it goes downward and, on the left, on an almost median plane. The bronchial, pericardial, oesophageal, intercostal and superior phrenic arteries originate from the descending thoracic aorta. The aorta finally bifurcates, at the level of the fourth lumbar vertebra, into the right and left common iliac arteries.
6.1.2.2 Pulmonary Artery
The common pulmonary trunk, or simply pulmonary artery, originates from the right ventricle; it goes upward for approximately 5 cm, anterior to the ascending aorta, and, below the aortic arch, it divides into the left and right branches.
The pulmonary artery is completely surrounded by the pericardium; it touches anteriorly the pleura and the left lung; posteriorly we find the ascending aorta and the left atrium.
The right and left pulmonary arteries, with a manly horizontal course, reach the lung through the hilum and divide into the lobar, segmental and subsegmental branches. The right pulmonary artery, slightly longer and wider than the left one, sends a ramification toward the superior lobe and gives rise to the interlobar branch; the branch for the middle and inferior lobes originates from the latter. The left pulmonary artery, slightly shorter and with a smaller diameter than the right one, reaches the pulmonary hilum and divides into two branches, for the superior and lower lobe; the latter sends a branch to the lingula. The pulmonary arteries carry deoxygenated blood from the heart to the lungs; they are the unique arteries carrying venous blood in the human body.
6.1.2.3 Thoracic Veins
The superior vena cava, collecting the venous blood from the upper part of the body, is originated by the merger of the left and right brachiocephalic veins (innominate veins); it drains into the superior part of the right atrium.
The inferior vena cava, carrying the venous blood from the lower part of the body into the inferior part of the right atrium, originates in the abdominal cavity, and it is formed by the joining of the left and right common iliac veins; after crossing the diaphragm, it enters the chest.
The azygos system consists of the right azygos vein, on the right, and hemiazygos and accessory hemiazygos veins on the left. The azygos vein runs up along the lumbar and dorsal spinal column, up to the fourth dorsal vertebra; it goes forward, drawing an arch toward to the superior vena cava; it receives blood also from the fourth to the eleventh posterior intercostal veins on the right side.
The hemiazygos vein climbs along the spinal column, up to the eighth dorsal vertebra, and collects the blood from the last three posterior intercostal veins on the left. The hemiazygos accessory vein ascends on the left side of the dorsal column and receives the posterior intercostal veins coming from the fourth to the eighth intercostal space. The hemiazygos and accessory hemiazygos veins may merge into the azygos one, independently, or through a common trunk.
The pulmonary veins are four, two superior ones (right and left) and two inferior ones (right and left); they all flow into the left atrium, carrying oxygenated blood from the lung to the heart; these are the only veins in the human body carrying arterial blood.
6.1.3 Heart
The heart, central organ of the circulatory system, is located in the mediastinum, between the lungs (Fig. 6.3). It looks like a conic trunk, flattened on the anterior-posterior line, with the base upward and the apex downward on the left. The major axis is oblique from the back to the front, from top to bottom and from right to left; the heart, therefore, is not in the centre of the symmetrical plane; 2/3 of its volume, in fact, peer out from the left. Some anatomical variations are considered normal, such as mesocardia, when the cardiac axis is vertical, and dextrocardia, when the cardiac apex is on the right; this last condition is often associated with the situs viscerum inversus.
The heart volume may vary and depends on sex and age; it is proportional to the size of the person and related to the weight and the body surface, rather than the height. In adults the heart weighs 280–340 g in men and 230–280 g in women.
It is protected by the sternum, anteriorly, and the costal cartilages (from the third to the sixth one), ensuring a safe protection from the outside. The posteroinferior face leans against the diaphragmatic vault, while above it continues into the great vessels of the cardiac pedicle, consisting of, from right to left: superior vena cava, ascending aorta and pulmonary arterial trunk.
The heart is contained in a fibroserous sac, the pericardium, that attaches it to the diaphragm and isolates it from the surrounding organs. The pericardium consists of two layers, the parietal and visceral layers; normally, the space between them is a merely virtual space and therefore not visible with the available imaging techniques; it is rather visible in case of interposition of a third element (such as pericardial effusion, either haematic or not) between the layers, which may occupy the virtual lumen. In view of the above, it is important to be reminded that the pericardium also covers the initial part of the great vessels of the cardiac pedicle and the pulmonary veins: it is therefore easy to understand how a traumatic event, fissurations or breakage of such structures, may lead to an acute intrapericardial haematic effusion with consequent cardiac tamponade.
Through the pericardium the heart enters into contact with the right lung, posteriorly, and with the organs adjacent to the posterior mediastinum, in particular with the oesophagus. This organ, along with the azygos vein, the thoracic duct, the vagus nerves and the descending aorta, separates the heart from the thoracic vertebrae, from the fifth to the eighth one, which are also named, for this reason, cardiac vertebrae.
On the external surface of the heart, we find the anterior face, or sternocostal face, the posteroinferior or diaphragmatic face, the base (to which the vessels of the pulmonary and systemic circulation are connected), the apex, which is oriented downward on the left, and the two margins, the right one, acute, and the left one, obtuse (Figs. 6.4 and 6.5).
Fig. 6.4
Anatomy of the heart, frontal view. Ao ascending tract of the thoracic aorta, AoA aortic arch, BCA brachiocephalic artery, IVC inferior vena cava, LAD descending anterior branch of the left coronary artery, LCC left common carotid artery, PA pulmonary artery, SA subclavian artery, SVC superior vena cava
Fig. 6.5
Anatomy of the heart, posterior view. AoA aortic arch, BCA innominate artery, IVC inferior vena cava, LCC left common carotid artery, PA pulmonary artery, left side, PDA posterior descending branch of the right coronary artery, PV pulmonary veins, left side, SA subclavian artery, SVC superior vena cava
The diaphragmatic face includes the atrioventricular groove (or coronary sulcus), which is transverse and separates the posterior-superior (or atrial) portion, from the anteroinferior, or ventricular, one; we also find the interatrial sulcus that, along with the posterior interventricular sulcus, delimits the external border of the four cardiac cavities. On the sternocostal and diaphragmatic faces, there are two longitudinal sulci, the anterior and the posterior one (also named interventricular sulci), going from the coronary sulcus to the apex of the heart. The atrioventricular groove and the interventricular sulcus are very important because they contain the coronary arteries.
The heart is a hollow organ, divided into two independent parts, the left and right parts, each of them consisting of two cavities: the superior cubic cavity, the atrium, and the inferior cavity, pyramidal or conical, the ventricle (Fig. 6.6).
Fig. 6.6
Anatomy of atria, ventricles and interventricular septum, oblique-longitudinal view. Ao ascending aorta, LA left atrium, LV left ventricle, PA pulmonary artery, PV pulmonary vein, RA right atrium, RV right ventricle, SVC superior vena cava
On the plane passing between the two atria and the ventricles, there is a fibrous structure, the so-called cardiac skeleton, namely, the insertion point of the bundles of the atrial and ventricular myocardium; this is the place where heart valves are placed, in order to ensure the structural continuity of the ventricles and the big arteries. There are four fibrous rings, on the border of the venous and arterial ostia, two fibrous trigones, interposed between the fibrous rings, the tendon of the conus arteriosus and the interventricular membranous septum.
The right atrium is anterior to the left one. It looks roughly a cube, with six walls. The anterosuperior wall coincides with the sternocostal face; the posterosuperior one with the heart base, where we can find the outlets of the venae cavae; the posteroinferior wall with the small diaphragmatic face receives the end of the coronary sinus; on the anteroinferior one we find right atrioventricular orifice; the medial wall consists of the interatrial septum, where we find the fossa ovalis, the remnant of a thin fibrous sheet that covered the foramen ovale; and lastly, the lateral wall has a hole of connection with the right auricula, and it is characterised by fleshy reliefs due to the presence of the musculi pectinati (they resemble the teeth of the comb, hence the name).
The right ventricle has a capacity of approximately 200 ml, and it looks like a pyramid with a triangular base and three walls: the anterior wall, corresponding to most of the sternocostal face of the heart; the posteroinferior wall, consisting of the right, less-extended portion of the diaphragmatic face of the heart; the medial or septal wall, consisting of the interventricular septum; the base has two orifices or ostia, a venous atrioventricular one, located on the right, in the back; and an arterious or pulmonary one, in the front on the left side, through which the ventricle communicates, respectively, with the right atrium and the pulmonary trunk.
The right atrioventricular orifice (or tricuspid orifice, or ostium atrioventriculare) is supplied by a valve (tricuspid valve) consisting of three leaflets called cusps. For their positions, the cusps are divided into medial, septal, anterior and posterior cusps; they consist of fibrous tissue, covered with endocardium. The free margins of the valvular leaflets, irregularly dentate, allow the insertion of the chordae tendineae (tendinous chords), thin tendons which are detached from the apex of the conical muscles, protruding into the cavity, called papillary muscles. The pulmonary orifice has three semilunar valves (membranous folds) that can be distinguished into anterior, right and left valves.
The right ventricular wall is thicker than the atrial wall but almost 1/3 thinner of the left ventricular wall.
The left atrium is less voluminous than the contralateral one, but its walls are thicker. We can distinguish six walls: anterosuperior wall, corresponding to the sternocostal face, in connection with the descending part of the aorta and the pulmonary trunk; posterosuperior wall, in relation with the oesophagus through the interposition of the pericardium; posteroinferior wall, less extended, corresponding to the diaphragmatic face; anteroinferior wall, with the atrioventricular orifice; medial wall, in correspondence of the interatrial septum; and the lateral one, providing access to the auricle.
The four pulmonary veins, two on each side, open up in the posterosuperior wall of the atrium, through four orifices, devoid of valves; however, they also have a high level of individual variability (Fig. 6.7).
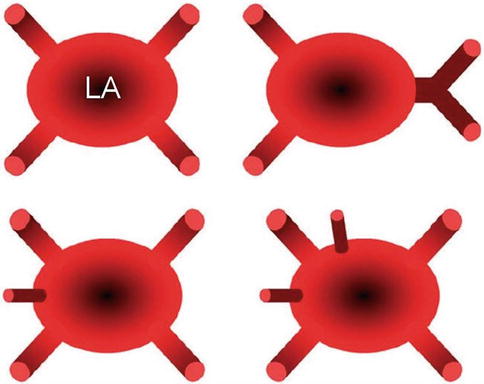
Fig. 6.7




Possible anatomical variations of the pulmonary veins when flowing into the left atrium. LA left atrium
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
