Localization: The most frequent locations are femur, tibia, humerus, and pelvis. Usually located in the meta-diaphysis, it may invade the epiphysis or be multicentric.
Clinical: In low-grade tumors, there is mild pain, no soft tissue mass, and a slow course. In high-grade fibrosarcoma, pain may be severe with a soft tissue mass, joint involvement, the course is rapidly progressive, and pathologic fracture is common.
Imaging: It is a purely osteolytic tumor with ill-defined limits, interruption of the cortex, and soft tissue mass. Periosteal reaction is scarce or absent. Low-grade tumors may present better-defined borders.
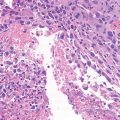
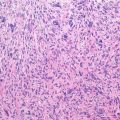
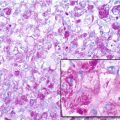
Histopathology: Fibrosarcoma tends to be firm and whitish when containing more collagen (low grade) and pink gray and soft to encephaloid, when the cells prevail (high grade). It is typically a spindle cell tumor with a rather uniform aspect throughout. The tumor is composed by spindle cells and collagen fibers. These form fascicles or streams, where cells are all oriented in the same direction (as a school of fish). Grading (from 1 to 4) is based on differentiation, number of cells, hyperchromatism, pleomorphism of nuclei, prominence of nucleoli, and frequency of mitoses. This grading has a clear bearing on treatment and prognosis.
Course and Staging: Generally, the course is slower as compared to OS. Grade 1 and 2 fibrosarcomas are staged I (low grade); grades 3–4 are staged II.
Treatment: Fibrosarcoma is resistant to radiotherapy. Preoperative chemotherapy is scarcely effective and not feasible in elderly patients. Often surgery cannot be as conservative as it is nowadays in OS.
Prognosis: Low-grade fibrosarcomas have a good prognosis with late metastases after a wide surgery. Stage II tumors demonstrate a high incidence of recurrences and metastases. The average survival rate at 10 years is around 30 %.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


