Figure 1.1.1
Gestational sac at 5.0 weeks of gestation: double sac sign. Sagittal midline view of the uterus demonstrates the gestational sac, which appears as a fluid collection (*) in the brighter mid-portion of the uterus (the decidua), with two echogenic rings around it. The inner ring (arrowheads) lies immediately adjacent to the fluid collection and completely surrounds it. The outer ring (arrows) partially surrounds the sac. Follow-up scan 6 weeks later demonstrated an 11-week fetus with heartbeat, confirming intrauterine pregnancy.
At approximately 5.5 weeks, the yolk sac, a circular structure that is normally <6 mm in diameter, is first identifiable within the gestational sac by transvaginal sonography (Figure 1.1.4). When scanning transabdominally, the gestational sac and the yolk sac are visualized approximately ½ week later than they are transvaginally.
The corpus luteum can usually be seen on ultrasound in one of the ovaries. It can have a number of sonographic appearances, including a simple cyst (Figure 1.1.5), a thick-walled or complex cyst, or a solid hypoechoic structure. It typically measures 2–3 cm in diameter.

Figure 1.1.2
Gestational sac at 5.0 weeks of gestation: intradecidual sign. Sagittal midline view of the uterus demonstrates the gestational sac, which appears as a fluid collection (*) in the brighter mid-portion of the uterus (the decidua). The sac lies beside a bright white line (arrowheads) running down the middle of the decidua, which corresponds to the collapsed uterine cavity. Follow-up scan 9 days later demonstrated an embryo with heartbeat, confirming intrauterine pregnancy.

Figure 1.1.3
Gestational sac at 5.0 weeks of gestation: “nonspecific” intrauterine fluid collection. Sagittal midline view of the uterus demonstrates the gestational sac, which appears as a fluid collection (*) in the brighter mid-portion of the uterus (the decidua). The sac does not demonstrate either the double sac sign or the intradecidual sign. Follow-up scan 10 days later demonstrated an embryo with heartbeat, confirming intrauterine pregnancy.
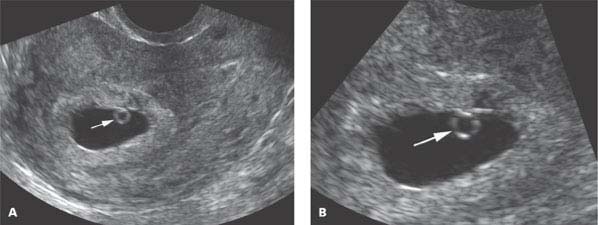
Figure 1.1.4
Gestational sac at 5.5 weeks of gestation. A: Sagittal midline view of the uterus demonstrates a yolk sac (arrow) within the gestational sac. B: Close-up view of the yolk sac in the gestational sac.

Figure 1.1.5
Corpus luteum. Transverse view of the uterus and right adnexa demonstrates a simple cyst in the right ovary, representing the corpus luteum (CL). The uterus, which is adjacent to the ovary, contains a gestational sac (arrow) with yolk sac (arrowhead).
1.2. Normal Pregnancy at 6–10 Weeks of Gestation
Description and Clinical Features
Between 6 and 10 weeks of gestation, the embryo undergoes rapid growth and development. It increases approximately 15-fold in length, from 2 mm at 6.0 weeks of gestation to 30 mm at 10.0 weeks. The internal organs differentiate, with organogenesis largely complete by 10 weeks. In particular, by 10 weeks, the cardiac chambers and valves are well formed, the gastrointestinal and genitourinary systems (which were joined at the urogenital sinus early in embryological development) are distinct, and the kidneys have begun their ascent from the pelvis.
The external appearance of the embryo also undergoes major changes during this stage. By 10 weeks, facial features are recognizable, and limbs, including fingers and toes, are formed.
During the 6–10-week time period, the chorionic villi at the implantation site proliferate whereas those opposite the implantation site regress. This results in two portions of the chorion: the thick chorion frondosum, where the villi have proliferated, and the smooth membranous chorion laeve, where the villi have degenerated. The chorion frondosum interdigitates with the maternal decidua to form the placenta. The thin smooth portion forms the chorionic membrane (often referred to simply as “the chorion”).
Sonography
The embryonic heartbeat can first be seen on transvaginal sonography at approximately 6.0 weeks of gestation. Initially, it is seen as a flickering movement adjacent to the yolk sac, with little or no distinct embryo identifiable (Figure 1.2.1). Within 2–3 days, the heartbeat can be seen to lie within a clearly visible embryo (Figure 1.2.2). The heart rate is normally at least 100 beats per minute before 6.3 weeks (corresponding to a crown-rump length [CRL] of <5 mm) and at least 120 beats per minute from 6.3 to 7.0 weeks (corresponding to a CRL of 5–9 mm).
The embryo initially appears on ultrasound as an undifferentiated structure, without identifiable parts (other than the beating heart). By 8 weeks, the head and trunk can be separately identified (Figure 1.2.3), and an intracranial cystic structure is identifiable, corresponding to the developing rhombencephalon (Figure 1.2.4). The body shape and proportions are considerably different from those of a newborn, in that the head is larger relative to the body and the neck is more flexed. By 9 weeks, the limbs have lengthened and limb motion can be identified (Figure 1.2.5).
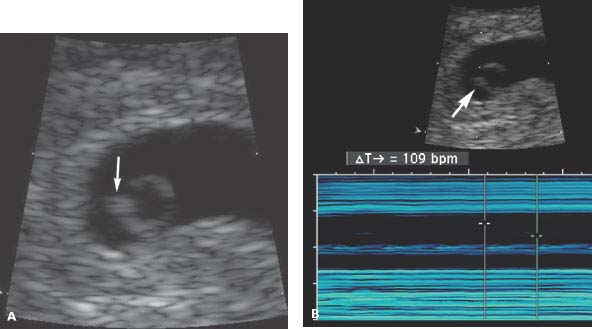
Figure 1.2.1
Embryonic cardiac activity at 6.0 weeks of gestation. A: The embryo (arrow) is barely visible, seen as a small area of thickening on the edge of the yolk sac. B: Cardiac activity in the embryo (arrow) is documented by M-mode to be at a rate of 109 beats per minute (calipers).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


