Fig. 6.1
Stereotactic body frame (Elekta): Patient setup using diaphragm control in SBRT. Breathing-related movement of tumor can be controlled
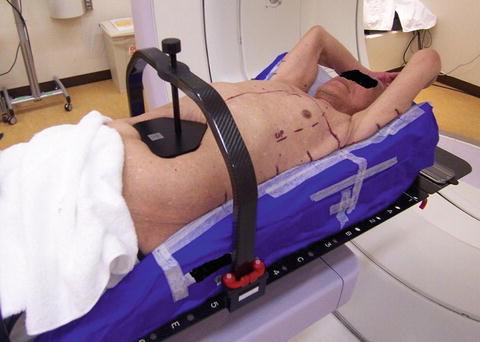
Fig. 6.2
Body FIX (Elekta): Patient setup using diaphragm control in SBRT

Fig. 6.3
Body FIX (Elekta): Patient setup in dynamic tracking irradiation. Positioning for dynamic tracking is setting in immobilization with free breathing condition, and the infrared marker is putting on upper abdomen for acquisition of breathing signal
To confirm breathing position, we placed an infrared marker [21, 22] on the diaphragm region with an abdominal pressure belt and observed the breathing pattern using a spirometer [13]. Accurate and reproducible fixation could be achieved using this device.
Breathing-related movement can be controlled by suppressing diaphragmatic movement as with an abdominal pressure board. Whether movement is restrained can be determined by observing tumor movement by fluoroscopy, and the strength of pressure applied by the board can be regulated accordingly.
In cases with a lesion in the lower lung field, diaphragm movement can be restrained by an average of more than 5 mm, and therefore the irradiation range can be minimized by reducing the movement of the tumor [15].
Depending on the case, breathing-related movement may be large when pressure is applied to the diaphragm region. Such movement may be controlled by applying abdominal pressure, but it may be necessary to apply oxygen inhalation as breathing tends to become relatively shallow with such treatment [7].
Then, I explain the function of the fixture with the change of the fixture of our facilities.
When we first began performing stereotactic body irradiation at our facilities during until 2007, we adopted the Stereotactic Body Frame (SBF) [1–6, 16] (Fig. 6.1) developed by the Swedish company Elekta with the cooperation of Karolinska Hospital in Stockholm.
We subsequently introduced the high-flexibility Body Fix [24, 25] (Fig. 6.3) for immobilization, which interfered little with the gantry and showed little dose absorption at our facilities.
Irradiation was carried out in patents under free-breathing conditions by dynamic tumor tracking irradiation [18–23]. It became clear that immobilization techniques with which it was easy to observe movement from each direction in fluoroscopy images were required.
This method is available for liver and pancreatic cancer, and clinical results have been reported for a therapeutic method using SBF adapted for body irradiation [1–6].
Figure 6.4 shows immobilization SBF for use in SBRT of the trunk region. The size and shape of SBF with a minimum opening of 550 mm are designed for CT, magnetic resonance (MR), and positron emission tomography (PET). The frame wall is composed of glass fiber and white birch plywood, low-density materials that keep attenuation of the beam to a minimum [16]. There is an atmospheric layer and a vacuum pillow inside the frame. CT level of pillow part is almost equivalent to atmosphere. This part can be molded along the body of the patient. Furthermore, a CT indicator made of polymethyl methacrylate (PMMA), which can read the three-dimensional coordinates on CT, is embedded within the inner wall of the frame, and a Z-axis scale made of plastic is attached to the outer wall. A XY- axis scale for positioning is shaped arch on a frame, and made of aluminum, which can remove during irradiation. There is a level control that made of rubber bag in unilateral of the frame base. This function can control to coordinate the position of horizontal direction with adjusting of air pressure. In addition, as other appliances, laser pointer can be set for skin marker on chest wall (Fig. 6.5a), and the pressure board can be set to control breathing movement on upper abdomen.
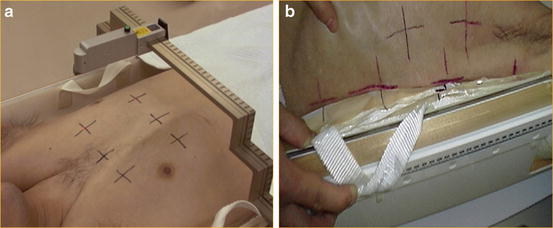
Fig. 6.4
Structure of SBF immobilization: (1) Body frame, (2) Chest marker, (3) Leg maker, (4) Level control, (5) Diaphragm control, (6) XY-axis scale, (7) localizer scale for CT image
Fig. 6.5
(a): Skin marking line on contact point with immobilization is useful for setup in every positioning. (b): Chest laser marker on SBF. In positioning, this marker is used for setting to prevent of leaning and twisting body
The stereotactic body frame (SBF) has many functions that were developed for stereotactic body radiation therapy (SBRT) with a high degree of reproducibility. We introduced Body Fix in place of SBF in our facilities in 2007 as it has a number of advantages in that it is composed of material with little dose absorption, its structure interferes little with the gantry, and it has high spatial flexibility. For dynamic tumor tracking irradiation, the patient is irradiated under free-breathing conditions. Therefore, a fixation device that facilitates observation of the movement of a marker and the lesion in fluoroscopy images during irradiation or verification was required. The fixation device requires precision, and a function to reproduce the setup position of bone exactly is required. Alignment requires use of a skin mark and an adjustment appliance prior to use. Bone position can be reproduced with greater precision and within a shorter time using image-guided radiation therapy (IGRT) compared to previous methodologies. The position revision in verification enabled automatic reproduction of a position and a tilt with accurate six-axial (X, Y, Z, Roll, Pitch, and Yaw) revision of couch position. However, during setup, it is necessary to reproduce torsion and flexure of the body in a minimum requirement. Accordingly introduction of IGRT, the purpose of the fixture and the necessary matter changed. Use of a fixation device such as Body Fix, which is simple and shows little absorption, is effective for positioning verification using fluoroscopy, such as dynamic tracking irradiation or irradiation synchronized with respiration.
6.4 Points That Require Attention in Immobilization
Long-term patient fixation may be accompanied by patient discomfort, with reduced blood circulation resulting in numbness. In addition, low back pain due to remaining in the same posture for a long time may occur. To prevent these issues, it is necessary to fix the patient in as relaxed a state as possible. It is comfortable for patient that neck and both elbows are lifted up naturally in making immobilization. It is easier for patients to remain in the same position for a long time when they are relatively comfortable, and this improves precision.
For immobilization, we do not begin alignment immediately as it is important to confirm the patient’s breathing and to perform the procedure with the patient in a relaxed state. This step must be performed manually in each case, and we explain the positioning procedure to the patient to secure his/her cooperation.
In the case of vacuum-type fixation, we should not be write mark and scan CT soon after making fixation. The patient is awakened after immobilization, and then the point of contact on the skin surface is marked to ensure application to the same position in each treatment (Fig. 6.5b). This can prevent extreme clamping and ensure that there are no differences in the conditions at the time of irradiation.
With regard to the time to irradiate, it is desirable to set as possible the same time in consideration of time after a meal.
In the case of using diaphragm control and shell on chest, there is some possible of deteriorating in precision of setup position, and cause to pain of the patient.
6.5 Immobilization and Setup Error
Due to the high dose of radiation given at each time, repositioning accuracy may influence the radiation dose applied to the lesion.
Patient fixation is closely related to intra- and interfractional setup error. The positional precision depends on accurate repositioning and maintenance of the patient’s position during irradiation. Positional precision is confirmed just before irradiation and any error is revised. It is necessary to maintain the position during treatment [26].
The introduction of IGRT technology has enabled bone position to be corrected just before irradiation, along with the position or tilt on X-ray images in six-axial directions, which can reduce the internal fractional setup error. However, we cannot revise the torsion of the body, curve, expansion, or contraction by IGRT revision. It leads to reducing internal fractional setup error to decrease these states by the setup using the fixture as much as possible. It is important that patient movement during irradiation remains within the bounds considered in intrafractional setup error, as outlined in the ICRU-62 report [27] regarding factors related to planning target volume (PTV).
It is important that the fixation device is capable of ensuring that the patient does not move during irradiation. Simultaneously, the fixation device must not be tight and uncomfortable to facilitate relaxation of the patient. If these conditions are satisfied, inter- and intra-fractional setup errors would be reduced, thus lowering the margin setting added to internal target volume (ITV).
Once immobilization has been achieved, adjoining regions of the skin are marked with lines (Fig. 6.5b). Lining up these marks on the right and left sides of the body can prevent rolling of the body axis.
When calvarial position accords in immobilization at the decided position, in the craniocaudal direction, the same position is reproduced every time. Therefore it is important to form the calvarial part of the fixture definitely.
The evaluation of repositioning is usually verified by bone position. For other methods, a tumor position is verified with higher precision by the observation of the internal marker using fluoroscopy or the verification of the organ using CBCT.
Agreement of tumor position according to the internal marker and CBCT increases the degree of positional precision, but changes in the trajectory of the irradiation beam and lesion depth affect the absorbed dose when there are changes in the body axis. Therefore, it is necessary to prevent changes in the body axis as much as possible because the fractional radiation dose is high.
For immobilization, it is necessary to achieve precise repositioning of the bone without leaning or twisting, and to ensure that the position can be maintained throughout treatment. The most suitable fixture choice is expected in consideration of an irradiation method, a collation method, irradiation time in each facility. I introduce the report about the setup error using various immobilization devices (Table. 6.1). An irradiation method and the collation methods are different in each report. For details, I suggest that you take each report into account.
Table 6.1
Setup accuracy using immobilization device for lung stereotactic body radiation therapy
Immobilization device | LAT (mm) | AP (mm) | SI (mm) | Reference |
|---|---|---|---|---|
Body fix with dual vacuum | 3.1 ± 2.6 | 3.4 ± 2.9 | 2.2 ± 1.9 | Luo [28] |
2.9 ± 3.3 | 2.3 ± 2.5 | 3.2 ± 2.7 | Fuss [29] | |
Body fix | −1.8 ± 3.2 | 0.3 ± 1.8 | 1.5 ± 3.7 | Wang [30] |
Stereotactic body frame | 6 | 4 | 7 | Negoro [15] |
3.3 | 3.4 | 4.4 | Wulf [6] | |
5 | 5 | 8 | Lax [2] | |
2.7 ± 2.3 | 2.5 ± 1.7 | 3.4 ± 2.7 | Inga [31]
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|