Case presentation
A 10-year-old female presents with 2–3 weeks of progressively worsening throat pain and dysphagia. She was diagnosed 2 weeks ago with Streptococcal pharyngitis by her primary care provider. She was treated with a 10-day course of amoxicillin and had mild improvement, but her symptoms returned. She was evaluated by her physician again and told she had a viral infection, since her rapid strep test was negative. Over the past 3–4 days, she has had fever to 103 degrees Fahrenheit; the throat pain and dysphagia have worsened considerably. Her parents note she has had “voice changes”—the child’s voice has taken on a “muffled” quality. She has had no other symptoms, has had no travel, and has been otherwise in her usual state of health.
Physical examination reveals an uncomfortable appearing child; she appears ill. She prefers to sit up, stating that lying down makes it “more difficult for me to breathe.” Her temperature is 101 degrees Fahrenheit, her heart rate is 120 beats per minute, respiratory rate is 25 breaths per minute, blood pressure is 120/80 mm Hg, and oxygen saturation is 95% on room air. She has an erythematous posterior oropharynx without obvious asymmetry, but her examination is limited secondary to difficulty opening her mouth, which she states hurts her throat. Her chest examination is clear, but there is transmitted upper airway noise. There is no obvious stridor.
Imaging considerations
Acutely ill, toxic-appearing children should have immediate treatment, including airway stabilization if clinically indicated. While having an imaging study to assist in diagnosis is advantageous, delaying care to obtain such a study is not advisable, since these children can decompensate quickly. Once a clinician deems it safe, then appropriate imaging studies may be performed.
Plain radiography
Plain radiography has the advantage of being readily accessible and providing relatively low ionizing radiation exposure. Anteroposterior and lateral views are usually performed. Depending on the etiology, plain radiography may demonstrate findings in certain clinical scenarios. For example, narrowing of the proximal trachea may be seen in croup (the classic “steeple sign”), radio-opaque foreign bodies may be visualized, and exudative tracheitis may show linear airway filling defects, irregularity, or asymmetric subglottic narrowing. , Interpretation of plain radiography should be performed in the context of the child’s history, clinical examination, and clinician suspicion for a particular disease process.
Computed tomography (CT)
CT can detect various pathologies, including tracheitis, epiglottitis, abscess, and foreign bodies. However, CT involves ionizing radiation exposure, and is not portable, requiring the patient to go to the CT scanner. In patients with potential airway compromise, this can complicate completing a CT study.
Magnetic resonance imaging (MRI)
MRI is not a first-line modality in the acutely ill patient. However, it is excellent at imaging anatomic and infectious causes of upper airway problems. Availability and the need for sedation are limiting factors to more immediate use.
Imaging findings
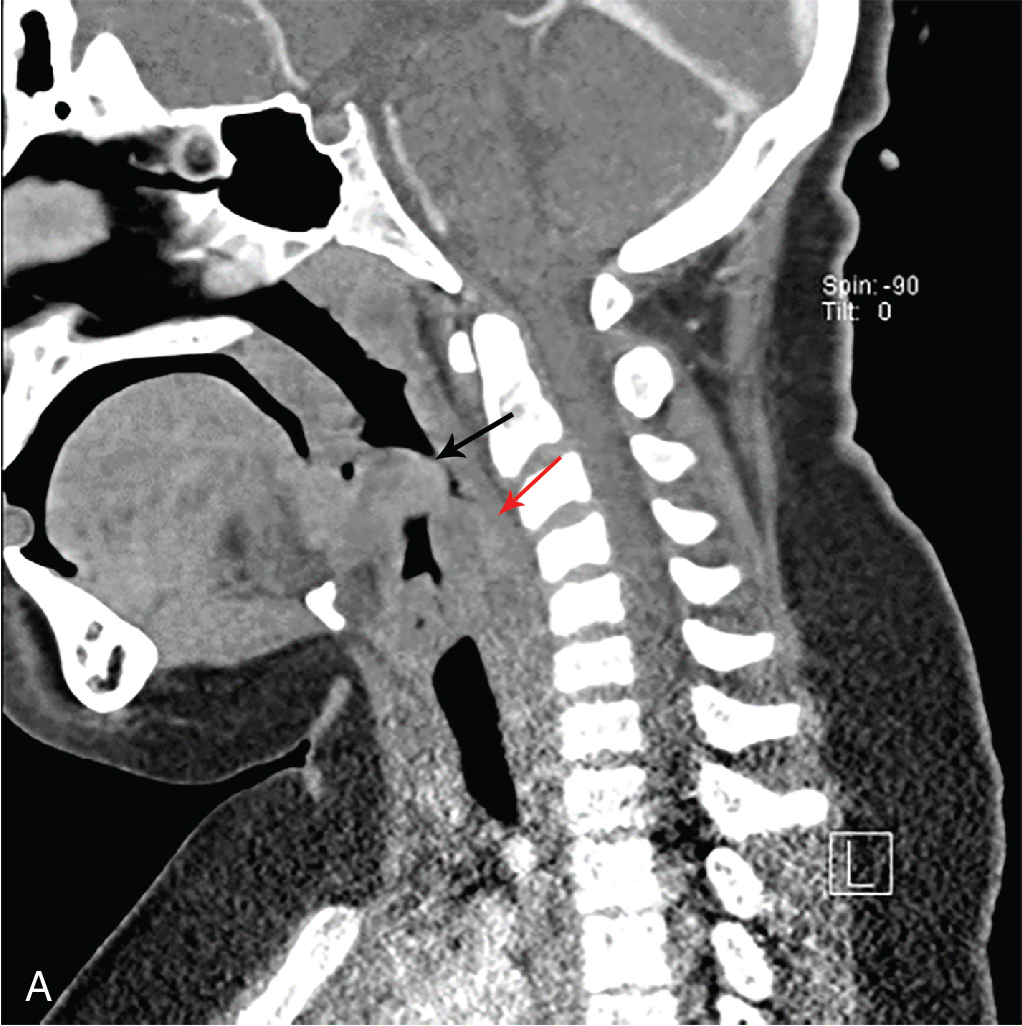
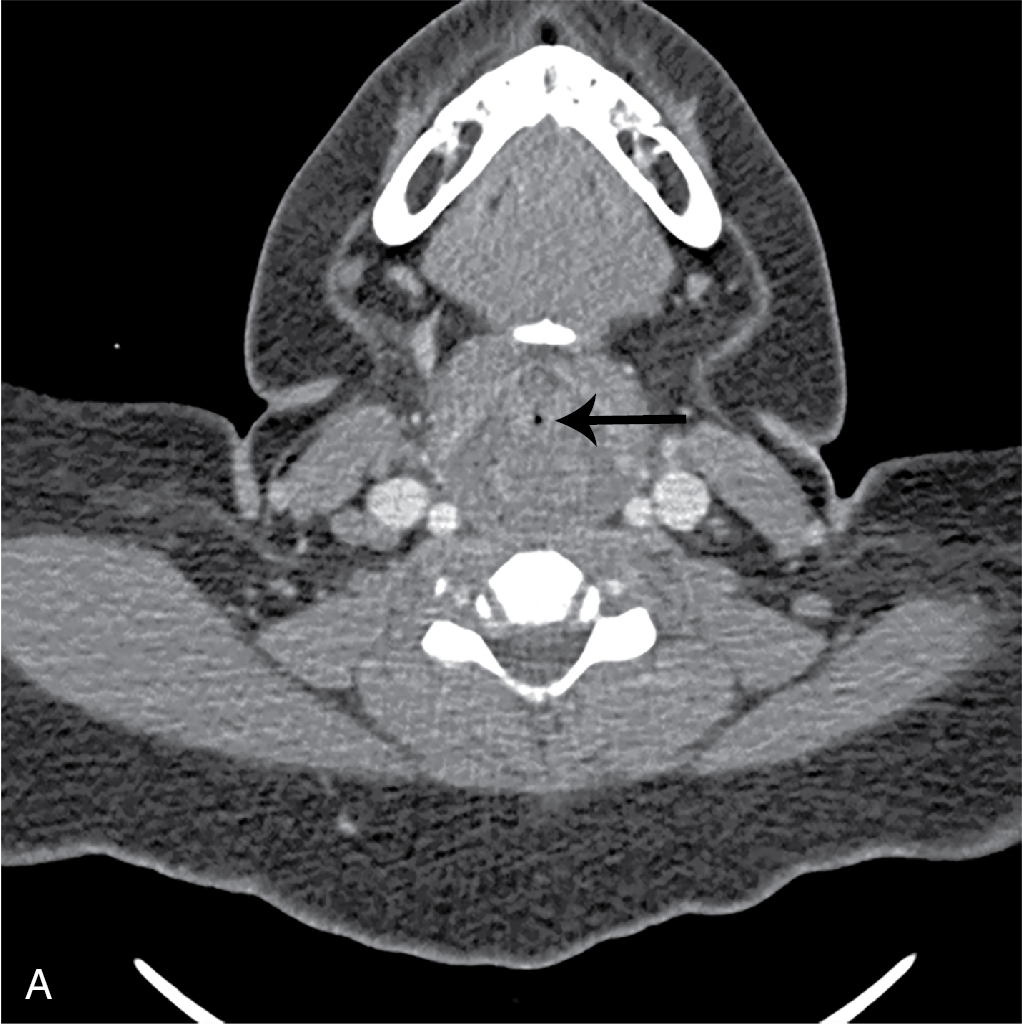
While the child did appear uncomfortable, she was deemed stable to undergo imaging. In this case, the decision was made to obtain an intravenous (IV) contrast–enhanced CT study of the soft tissues of the neck. Selected images are provided. There is no evidence of abscess, but there is diffuse edema in the hypopharyngeal and laryngeal region extending along the visualized upper trachea, producing severe airway narrowing, greatest in the hypopharyngeal and laryngeal regions. These findings are consistent with severe supraglottic swelling ( Figs. 83.1 A, 83.2 A and 83.3 A). For comparison, CT images demonstrating normal views of these structures are provided ( Figs. 83.1 B, 83.2 B, and 83.3 B).