1 Functional Anatomy of the Knee Joint
The knee joint (articulatio genus) is the largest synovial joint in the human body. Joint articulation is formed by the pairs of femoral and tibial condyles together with the menisci between them. In terms of arthrokinematics, this creates a joint with two axes that may be divided functionally into a meniscotibial and a meniscofemoral compartment. The saddle joint located between the patellar surface of the femur and the patella completes the knee joint (Fig. 1.1).
Joint Mechanics
Flexion, Extension, Rotation
The knee joint can be flexed or extended around a transversal axis passing through the femoral condyles. These movements occur primarily in the meniscofemoral compartment of the joint.
At flexion of about 30° and greater, the knee joint can be rotated inwardly or outwardly. Compared to the range of motion possible in flexion and extension, however, this degree of arbitrary rotation, occurring chiefly in the meniscotibial compartment, is low. The rotational axis connects the centers of the medial femoral condyle and medial tibial condyle.
The “Screw-home Mechanism”
There is a second, fundamental rotation that occurs automatically during the last 30° of extension. The so-called “screw-home mechanism” (knee-locking mechanism), produced by the varying diameters of the femoral condyles, causes an inward rotation of the femur of the standing leg of around 5° against the tibia, which is held in place by the weight of the body. This holds the knee joint in a locked position, i.e., the articular surfaces obtain a position of almost complete congruence. The fully extended knee is thus held in place only by the action of the joint, i.e., without any muscular activity, forming an integral component in the so-called amuscular standing posture.
“Unlocking” the knee from this position and resuming flexion requires the action of the popliteus muscle (see Figs. 1.6, 1.7, 1.9), a small and almost trivial muscle. Located deep in the hollow behind the knee (popliteal fossa), this muscle arises from the medial two-thirds of the dorsal aspect of the tibia, proximal to the soleal line. It attaches to the lateral and dorsal rim of the lateral meniscus and to the lateral femoral epicondyle. When the popliteus muscle contracts at the beginning of knee flexion, it pulls the lateral meniscus slightly dorsally while rotating the femur outwardly. This motion eliminates the congruence between the joint surfaces, freeing the femoral and tibial condyles to move against one another and the menisci.
Bony Structures
Femur (Fig. 1.1)
 joint surfaces on the medial and lateral condyles, as well as on the patellar surface of the femur, are covered with hyaline cartilage
joint surfaces on the medial and lateral condyles, as well as on the patellar surface of the femur, are covered with hyaline cartilage
 larger diameter of medial condyle (anteroposteriorly and proximodistally) than lateral condyle, the former serving as the center of voluntary rotation in the flexed knee
larger diameter of medial condyle (anteroposteriorly and proximodistally) than lateral condyle, the former serving as the center of voluntary rotation in the flexed knee
 the nonarticular condylar surfaces facing the intercondylar fossa serve as attachment sites for the cruciate ligaments (see below)
the nonarticular condylar surfaces facing the intercondylar fossa serve as attachment sites for the cruciate ligaments (see below)
 medial and lateral epicondyles as attachment sites for the collateral ligaments and the lateral epicondyle as insertion site of the popliteus muscle
medial and lateral epicondyles as attachment sites for the collateral ligaments and the lateral epicondyle as insertion site of the popliteus muscle
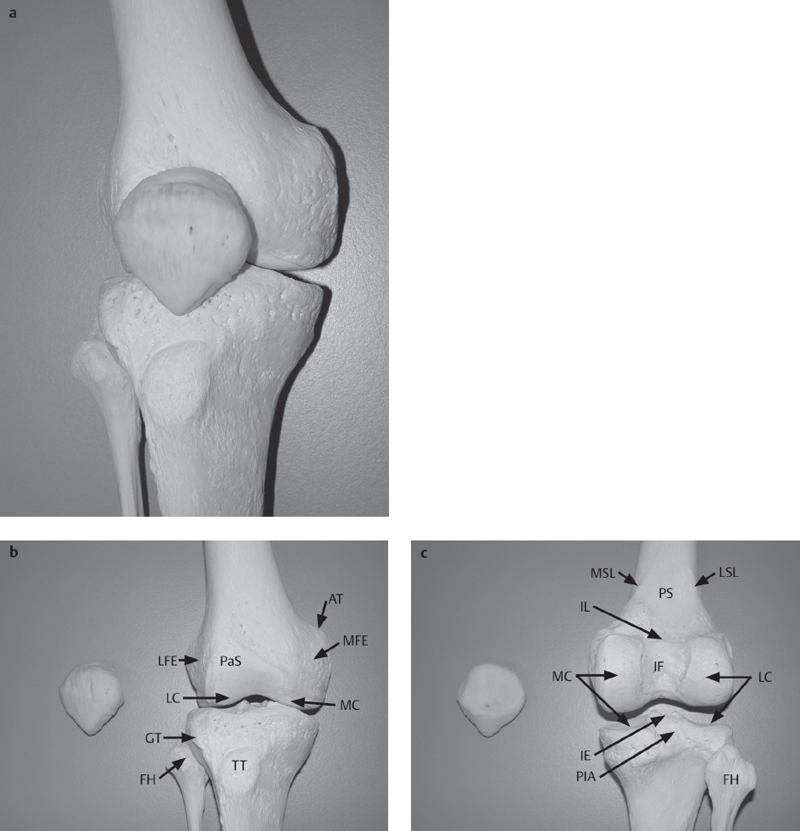
Fig. 1.1 a–c  Osteology of the femur and patella.
Osteology of the femur and patella.
Knee joint structures and surrounding structures demonstrated on elements of the lower limb skeleton of an adult male.
a, b View from anterior
c View from posterior.
AT | adductor tubercle |
FH | fibular head |
CT | Gerdy tubercle |
IE | intercondylar eminence |
IF | intercondylar fossa |
IL | intercondylar line |
LC | lateral femoral (tibial) condyle |
LFE | lateral femoral epicondyle |
LSL | lateral supracondylar line |
MC | medial femoral (tibial) condyle |
MFE | medial femoral epicondyle |
MSL | medial supracondylar line |
PaS | patellar surface |
PIA | posterior intercondylar area |
PS | popliteal surface |
TT | tibial tuberosity |
 articular surfaces on medial and lateral condyles covered with hyaline cartilage
articular surfaces on medial and lateral condyles covered with hyaline cartilage
 anterior intercondylar area as attachment site for the anterior cruciate ligament (ACL) as well as for the infra-patellar fat pad (Hoffa’s fat pad)
anterior intercondylar area as attachment site for the anterior cruciate ligament (ACL) as well as for the infra-patellar fat pad (Hoffa’s fat pad)
 intercondylar eminence as site of attachment for the anterior and posterior meniscal horns: medial meniscus at the medial intercondylar tubercle and lateral meniscus at the lateral intercondylar tubercle
intercondylar eminence as site of attachment for the anterior and posterior meniscal horns: medial meniscus at the medial intercondylar tubercle and lateral meniscus at the lateral intercondylar tubercle
 posterior intercondylar area and upper central posterior surface of tibia as attachment sites of the posterior cruciate ligament (PCL)
posterior intercondylar area and upper central posterior surface of tibia as attachment sites of the posterior cruciate ligament (PCL)
 tibial tuberosity as an insertion site for the patellar ligament, the distal prolongation of the quadriceps aponeurosis
tibial tuberosity as an insertion site for the patellar ligament, the distal prolongation of the quadriceps aponeurosis
 Gerdy tubercle on the anterior side of the lateral condyle anchoring the iliotibial tract, the reinforced part of the fascia lata
Gerdy tubercle on the anterior side of the lateral condyle anchoring the iliotibial tract, the reinforced part of the fascia lata
 “tuberculum tendinis” on the posterior aspect of the medial condyle: main attachment of the semimembranosus muscle (see Figs. 1.7, 1.8)
“tuberculum tendinis” on the posterior aspect of the medial condyle: main attachment of the semimembranosus muscle (see Figs. 1.7, 1.8)
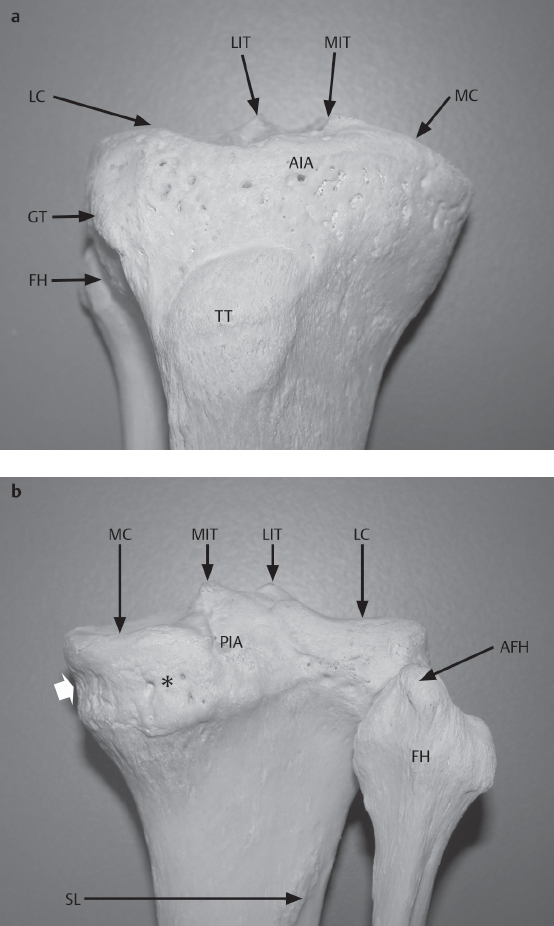
Fig. 1.2 a, b  Osteology of the tibia and fibula.
Osteology of the tibia and fibula.
Knee joint structures and surrounding structures demonstrated on elements of the lower limb skeleton of an adult male. Note the clearly visible “tuberculum tendinis” (asterisk) on the posterior surface and the groove (broad arrow) on the medial aspect of the medial condyle: both structures are caused by the insertion tendon of the semimembranosus (see also Figs. 1.7, 1.8)
a View from anterior.
b View from posterior.
AFH | apex of the fibular head |
AIA | anterior intercondylar area |
FH | fibular head |
LC | lateral tibial condyle |
LIT | lateral intercondylar tubercle |
MC | medial tibial condyle |
MIT | medial intercondylar tubercle |
PIA | posterior intercondylar area |
SL | soleal line |
TT | tibial tuberosity |
 largest sesamoid bone in the human body, embedded in the quadriceps aponeurosis
largest sesamoid bone in the human body, embedded in the quadriceps aponeurosis
 anterior (nonarticular) surface is grooved from the pulling forces exerted by the superficial fibers of the quadriceps tendon, which pass directly into the patellar ligament; not infrequently, chamberlike bony processes guiding the tendon fibers may occur as an anatomic variant
anterior (nonarticular) surface is grooved from the pulling forces exerted by the superficial fibers of the quadriceps tendon, which pass directly into the patellar ligament; not infrequently, chamberlike bony processes guiding the tendon fibers may occur as an anatomic variant
 posterior (articular) surface of the patella covered by a thick layer of hyaline cartilage
posterior (articular) surface of the patella covered by a thick layer of hyaline cartilage
 the base of the patella is directed proximally, while the apex, which also serves as attachment for the deep fibers of the patellar ligament, is pointed distally
the base of the patella is directed proximally, while the apex, which also serves as attachment for the deep fibers of the patellar ligament, is pointed distally
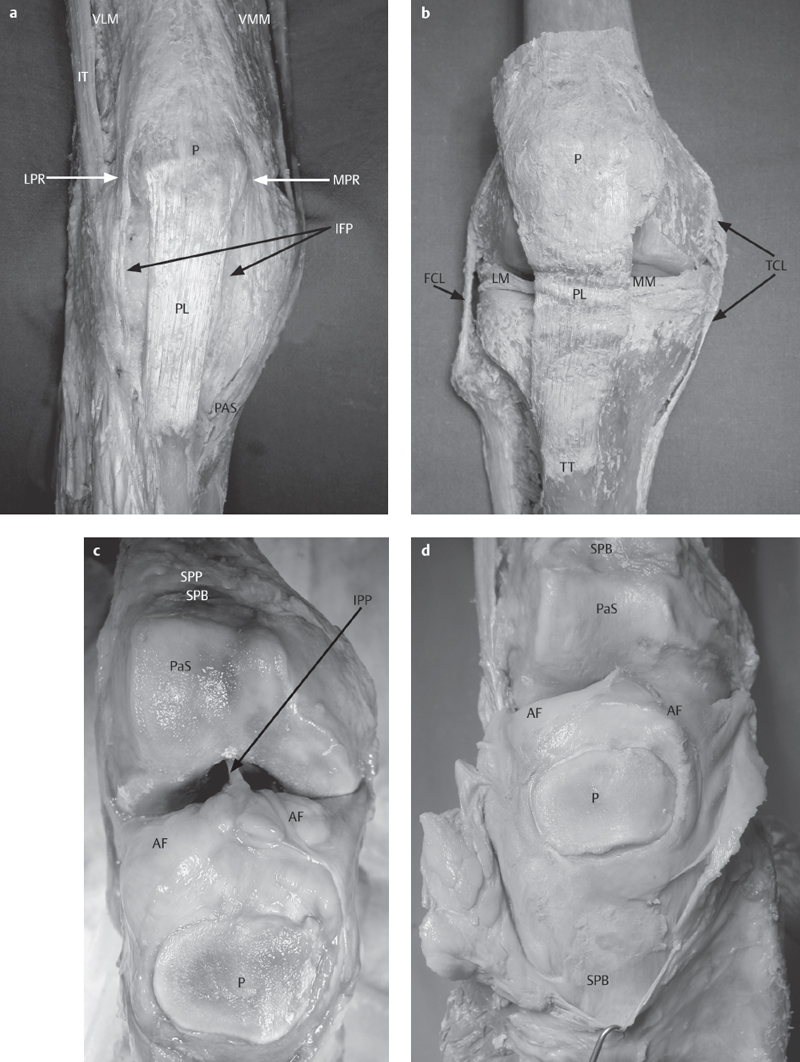
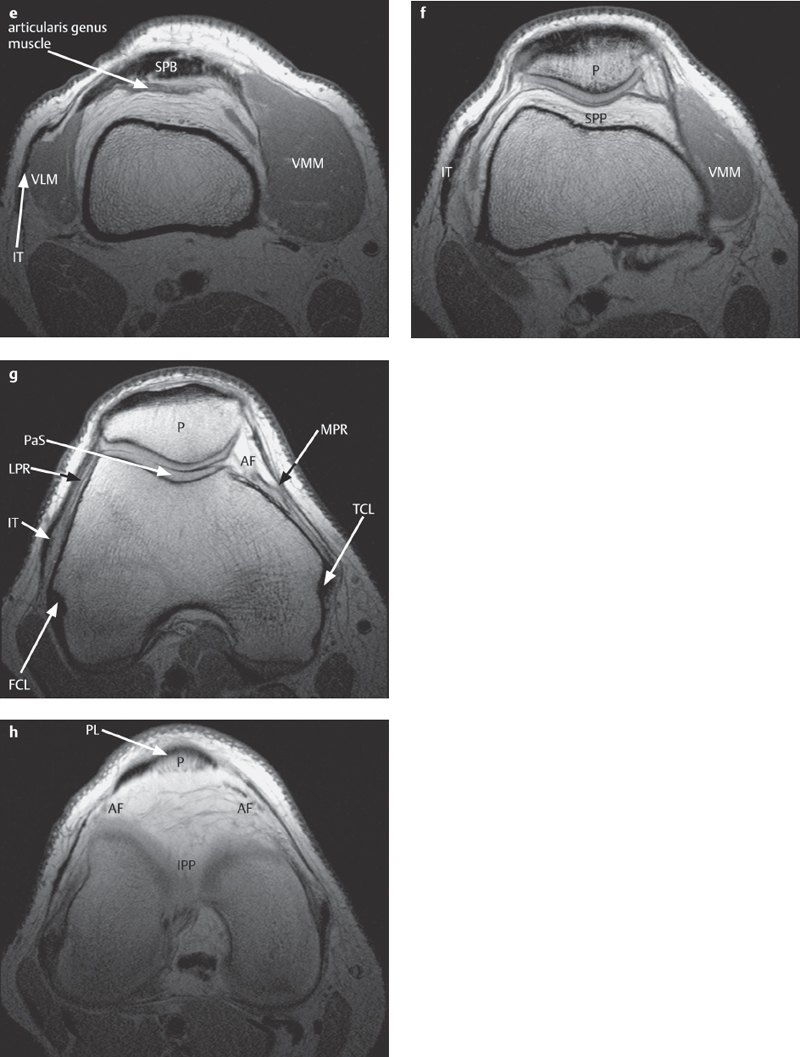
Fig. 1.3 a–h  Anterior components of the fibrous capsule, patellofemoral joint, and infrapatellar fat pad.
Anterior components of the fibrous capsule, patellofemoral joint, and infrapatellar fat pad.
a Superficial structures of the fibrous capsule. The nonreinforced parts of the fibrous capsule between the patellar retinacula and the patellar ligament have been removed to expose the underlying infrapatellar fat pad (IFP; Hoffa’s fat pad).
b Specimen of the right knee. All capsule-reinforcing muscular tendons were removed in order to demonstrate the main ligaments in relation to the menisci. Note the large distance between the lateral meniscus and the fibular collateral ligament, which runs outside of the fibrous capsule.
c Specimen of the right knee, opened from anterior. On the anterior wall of the joint, the infrapatellar fat pad (AF/IPP) creates a large gliding surface for both femoral condyles. Note the course of the infrapatellar plica (IPP), extending to the anterior of the intercondylar fossa and covering the anterior cruciate ligament. Proximal to the patellar surface (PaS) one sees the dorsal wall of the suprapatellar bursa (SPB), which is closed off by the suprapatellar plica (SPP).
d Specimen of the right knee. The quadriceps tendon can be seen forming the anterior wall of the suprapatellar bursa (SPB), which extends far proximally on the anterior aspect of the femur.
e Plain PD axial image of the suprapatellar bursa (SPB). The articularis genus muscle, formed by deep distal fibers of the vastus medialis muscle, is inserted into the suprapatellar plica preventing impingement of that synovial fold during knee extension.
f Plain PD axial image of the proximal region of the patellofemoral joint. With increasing extension, the proximal components of the patella meet the suprapatellar plica (SPP), which forms a gliding surface for the patella on the anterior surface of the femur proximal to the patellar surface (PaS).
g Plain PD axial imageofthe central portion of the patellofemoral joint. The lateral and central components of the patella (P) glide exclusively on the patellar surface (PaS), while the smaller medial articular surface of the femur is augmented by the ipsilateral alar folds (AF).
h Plain PD axial image of the infrapatellar fat pad. Note both lateral alar folds (AF) and the central infrapatellar plica (IPP) extending on the anterior surface of the anterior cruciate ligament.
FCL | fibular collateral ligament |
IT | iliotibial tract |
LM | lateral meniscus |
LPR | lateral patellar retinaculum |
MM | medial meniscus |
MPR | medial patellar retinaculum |
PAS | pes anserinus superficialis |
PL | patellar ligament |
TCL | tibial collateral ligament |
TT | tibial tuberosity |
VLM | vastus lateralis muscle |
VMM | vastus medialis muscle |
Fabella (Fig. 1.4)
 generally comprised of fibrocartilage, only seldom of purely bony material, forms additional sesamoid “bone” in the lateral head of the gastrocnemius muscle
generally comprised of fibrocartilage, only seldom of purely bony material, forms additional sesamoid “bone” in the lateral head of the gastrocnemius muscle
 articulates with the posterior surface of the lateral femoral condyle
articulates with the posterior surface of the lateral femoral condyle
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


