4
Gallbladder
Gallbladder Disease
Overview
 Cholesterol gallstones (85%) are the most common
Cholesterol gallstones (85%) are the most common
• Risk factors: Four Fs (female, fertile, fat, and forty)
• Due to imbalance between bile, lecithin, and cholesterol
 Pigmented stones (15%)
Pigmented stones (15%)
• Risk factors: Hemolytic disorders, biliary tract infection, ileal resection, cirrhosis
Definitions
Acute cholecystitis—inflammation of the gallbladder from stone impaction in the cystic duct
Choledocholithiasis—gallstone in the common bile duct which may lead to cholangitis
Signs and Symptoms
 Acute cholecystitis—leukocytosis and right upper quadrant pain
Acute cholecystitis—leukocytosis and right upper quadrant pain
• Murphy’s sign: Deep palpation of the liver edge during inspiratory phase worsens the pain, causing patient to cease inspiration
 Choledocholithiasis/ascending cholangitis
Choledocholithiasis/ascending cholangitis
• Charcot’s triad: Fever, jaundice, and right upper quadrant pain
• Reynold’s pentad: Charcot’s triad + altered mental status + shock
Diagnosis
 Ultrasound is the test of choice with high sensitivity and specificity
Ultrasound is the test of choice with high sensitivity and specificity
• Acute cholecystitis
 Gallbladder wall thickening (greater than 3 mm), gallbladder distension (greater than 10 × 4 cm), pericholecystic fluid, gallstone impacted in the cystic duct, and sonographic Murphy’s sign (Murphy’s sign pressing the ultrasound probe over the visualized gallbladder).
Gallbladder wall thickening (greater than 3 mm), gallbladder distension (greater than 10 × 4 cm), pericholecystic fluid, gallstone impacted in the cystic duct, and sonographic Murphy’s sign (Murphy’s sign pressing the ultrasound probe over the visualized gallbladder).
 Evaluate common bile duct size to determine if there is dilatation and/or choledocholithiasis
Evaluate common bile duct size to determine if there is dilatation and/or choledocholithiasis
• HIDA scan can be helpful if findings are not definitive on ultrasound
 Non-visualization of the gallbladder even after administering morphine (which closes the Sphincter of Oddi)
Non-visualization of the gallbladder even after administering morphine (which closes the Sphincter of Oddi)
Treatment
 Symptomatic cholelithiasis, biliary dyskinesia—elective laparoscopic cholecystectomy
Symptomatic cholelithiasis, biliary dyskinesia—elective laparoscopic cholecystectomy
 Acute cholecystitis—antibiotics, laparoscopic cholecystectomy
Acute cholecystitis—antibiotics, laparoscopic cholecystectomy
• Percutaneous cholecystostomy tube for ICU patients or patients who cannot tolerate surgery
 Choledocholithiasis, ascending cholangitis—endoscopic retrograde cholangiopancreatography (ERCP)
Choledocholithiasis, ascending cholangitis—endoscopic retrograde cholangiopancreatography (ERCP)
• Percutaneous transhepatic tube placement if ERCP is not available or if patient’s anatomy does not allow for ERCP
 Indications for intraoperative cholangiogram
Indications for intraoperative cholangiogram
• Previous history of choledocholithiasis, elevated liver function tests, gallstone pancreatitis
• Ultrasound showing dilated biliary duct
• Uncertainty of the anatomy during cholecystectomy
Other Important Facts
 Gallbladder wall calcification (porcelain gallbladder)—Perform cholecystectomy due to increased risk of gallbladder cancer
Gallbladder wall calcification (porcelain gallbladder)—Perform cholecystectomy due to increased risk of gallbladder cancer
 Gallbladder polyp—Perform cholecystectomy for patients who are symptomatic, polyps >1 cm, in patients greater than 50 years old, fast-growing/sessile polyps
Gallbladder polyp—Perform cholecystectomy for patients who are symptomatic, polyps >1 cm, in patients greater than 50 years old, fast-growing/sessile polyps
 Be mindful of gallbladder adenocarcinoma presenting acutely. Look for signs of an invasive gallbladder fossa mass, liver invasion or metastases, and lymphadenopathy.
Be mindful of gallbladder adenocarcinoma presenting acutely. Look for signs of an invasive gallbladder fossa mass, liver invasion or metastases, and lymphadenopathy.
RADIOLOGY
Acute Cholecystitis
 US findings (Fig. 4.1)
US findings (Fig. 4.1)
• Gallbladder distention with dimensions greater than 10 × 4 cm
• Pericholecystic fluid
• Gallbladder wall thickening greater than 3 mm
• Positive sonographic Murphy’s sign (the most specific finding)
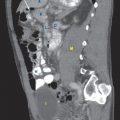
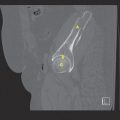
 CT findings
CT findings
• Gallbladder wall thickening and distention
• Pericholecystic fluid
• Fat stranding around gallbladder
• Gallstones are seen in minority of cases as either high- or low- density masses
 HIDA findings
HIDA findings
• Nonvisualization of gallbladder resulting from cystic duct obstruction
• Imaging performed 2 to 4 hours after administration of tracer, sometimes with the administration of morphine (which closes the Sphincter of Oddi to improve sensitivity)
FIGURE 4.1 A,B

FIGURE 4.1 A




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


