• Risk factors for malignancy: Age > 60, gallstones, coexistence of primary sclerosing cholangitis (PSC)
• Reassuring factors: Stability over time, multiple polyps, pedunculated (versus sessile) morphology
• Current recommendations
Cholecystectomy if patient is symptomatic or has cholelithiasis or PSC (regardless of polyp size)
Polyp > 18-20 mm: Open cholecystectomy
Polyp 10-20 mm: Laparoscopic cholecystectomy
Polyp 6-9 mm: Serial follow-up at 3, 6, and 12 months
Polyp ≤ 5 mm: Serial imaging (no consensus; malignancy is extremely rare and some advocate no follow-up)
(Left) Ultrasound of a 43-year-old woman with right upper quadrant pain shows mild gallbladder (GB) wall thickening and multiple small (< 5 mm), slightly echogenic polyps . An elective laparoscopic cholecystectomy for presumed biliary colic revealed cholesterolosis and cholesterol polyps.
(Right) Ultrasound image shows multiple polyps in the GB that measure < 1 cm in size. While the data suggests nodules < 1 cm harbor a very low risk of malignancy, most society guidelines suggest imaging follow-up.
(Left) Ultrasound of a 41-year-old man with chest pain shows two 4-mm GB polyps . Their small size, echogenicity, multiplicity, and stability at follow-up sonography indicate hyperplastic (cholesterol) polyps.
(Right) Ultrasound of a 47-year-old woman shows a 1-cm, pathologically confirmed adenomatous polyp . The likelihood of neoplasia increases with polyp size, but most GB polyps are hyperplastic.
TERMINOLOGY
Definitions
• Polypoid or sessile mass protruding from gallbladder (GB) mucosa
IMAGING
General Features
• Best diagnostic clue
Nonmobile hyperechoic mass protruding from GB mucosa without acoustic shadowing
• Location
GB lumen
• Morphology
Sessile or pedunculated
Imaging Recommendations
• Best imaging tool
Ultrasound; endoscopic ultrasound (EUS)
• Protocol advice
Grayscale and color Doppler US with 6 MHz transducer
CT Findings
• Often difficult to visualize on CT due to lower spatial resolution
CT underestimates polyp size compared to US
• Best visualized on CECT due to vascularity of polyp
Can show variable enhancement
No convincing evidence that polyp enhancement pattern predicts malignancy
• Ill-defined margins of larger polyps possible predictor of malignancy
• Useful for local staging (including lymph node metastases, liver invasion, metastases) in larger polyps where risk of malignancy is high
Ultrasonographic Findings
• Ultrasound is insensitive (only 50%) for polyps, detecting only 1/2 of polyps found at histopathology
• False-positive rate of up to 30%, with positive predictive value of only 10% (compared to histopathology)
Poor accuracy rates for polyps < 5 mm
Potentially due to stones, GB folds, sludge, or cholesterolosis mimicking polyps
Roughly 10% of polyps disappear on follow-up ultrasounds
– Original polyp may have been spurious, but could also reflect polyps breaking off or resolution of inflammatory polyps
• Immobile echogenic mucosal excrescence/nodule, either sessile or lobulated
No acoustic shadowing, unlike stones
Highly echogenic foci or “comet tail” artifacts within polyp suggests a cholesterol polyp
Large polyps may show internal vascularity on color Doppler US
No clear sonographic features to differentiate benign and malignant polyps
– Questionable link between sessile morphology and malignancy
– Multiple nodules more likely to be benign (usually cholesterol polyps); neoplastic polyps often solitary
• EUS has been shown to have higher accuracy in differentiation of benign (97%) vs. malignant (76%) polyps
Better demonstration of mucosal invasion
Only gold members can continue reading. Log In or Register to continue















 . An elective laparoscopic cholecystectomy for presumed biliary colic revealed cholesterolosis and cholesterol polyps.
. An elective laparoscopic cholecystectomy for presumed biliary colic revealed cholesterolosis and cholesterol polyps.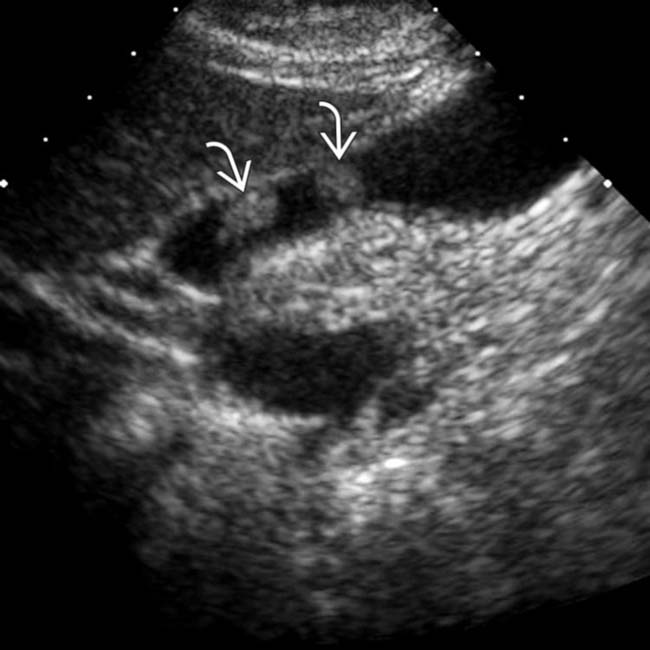
 in the GB that measure < 1 cm in size. While the data suggests nodules < 1 cm harbor a very low risk of malignancy, most society guidelines suggest imaging follow-up.
in the GB that measure < 1 cm in size. While the data suggests nodules < 1 cm harbor a very low risk of malignancy, most society guidelines suggest imaging follow-up.
 . Their small size, echogenicity, multiplicity, and stability at follow-up sonography indicate hyperplastic (cholesterol) polyps.
. Their small size, echogenicity, multiplicity, and stability at follow-up sonography indicate hyperplastic (cholesterol) polyps.
 . The likelihood of neoplasia increases with polyp size, but most GB polyps are hyperplastic.
. The likelihood of neoplasia increases with polyp size, but most GB polyps are hyperplastic.




















