and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
9.1 Case 1: Gastric Poorly Differentiated Adenocarcinoma
History
A 40-year-old male who was diagnosed to have gastric poorly differentiated adenocarcinoma after endoscopic biopsy underwent 18F-FDG PET/CT for staging.
Findings
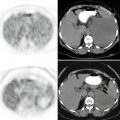
Fig. 9.1
Axial CT and PET images show intensely increased FDG uptake at gastric wall thickening (SUVmax 17.7) (a, b), hypermetabolic sclerotic lesions at pelvic bones are seen on CT and fusion images (SUVmax 5.9) (c, d)
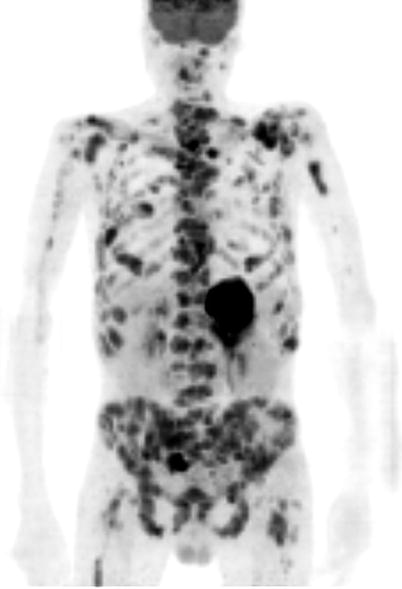
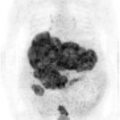
Fig. 9.2
MIP image show widespread hypermetabolic lesions at skeletal system as well as increased FDG uptake at gastric wall
Interpretation
Primary gastric malignancy with multiple metastatic lesions at skeletal system.
Teaching Point
The role of 18F-FDG PET/CT in pretreatment staging of gastric cancer is limited due to its low sensitivity for primary tumor and lymph node metastasis but it has the advantage of detecting distant solid organ and skeletal metastases by evaluating whole-body at one time.
9.2 Case 2: Gastric Adenocarcinoma and Virchow’s Node
History
A 60-year-old male who was diagnosed to have gastric adenocarcinoma after endoscopic biopsy underwent 18F-FDG PET/CT for staging.
Findings
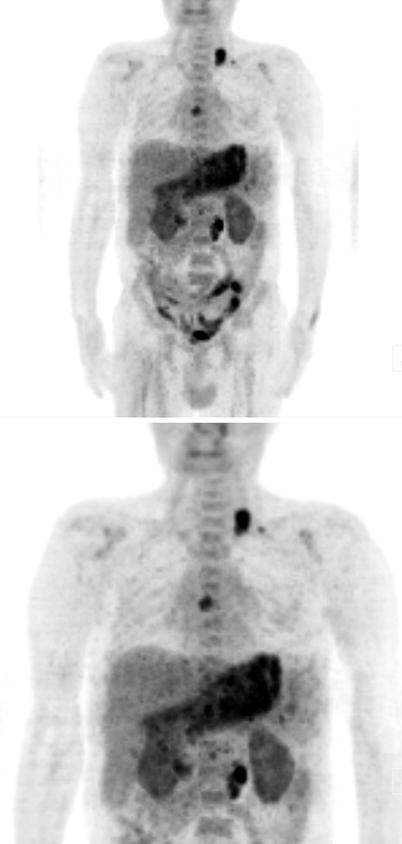
Fig. 9.3
MIP image shows moderately increased FDG uptake at stomach. There are hypermetabolic lymph nodes at subcarinal (SUVmax 6.4), left supraclavicular (SUVmax 8.8), paragastric, hepatogastric, and paraaortic (SUVmax 7.4) lymph node stations
Fig. 9.4
Axial CT and fusion images show moderately increased FDG uptake at gastric walls (a, b), hypermetabolic lymph node at left supraclavicular area (c, d)
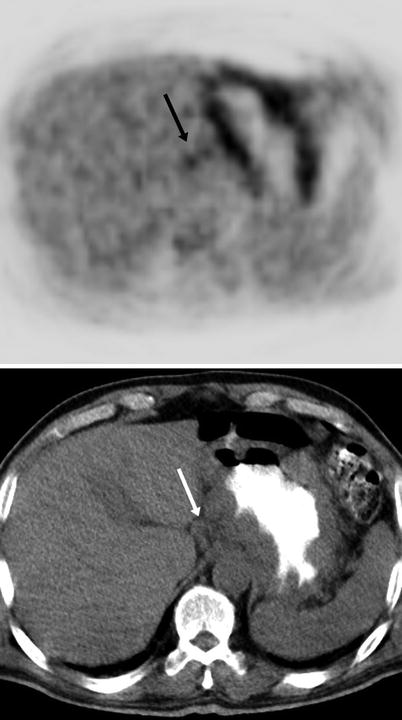
Fig. 9.5
Axial PET and CT images show mildly increased FDG uptake at hepatogastric lymph nodes (arrow)
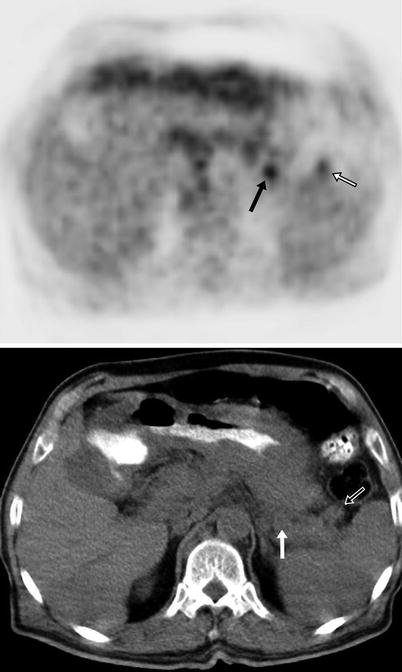
Fig. 9.6
Axial PET and CT images show mildly increased FDG uptake at paragastric lymph nodes (arrows)
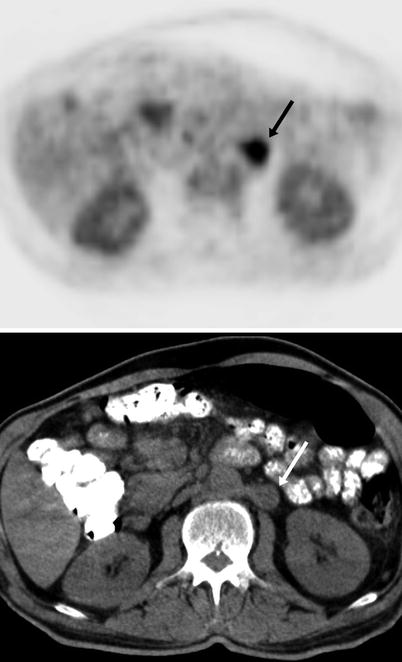
Fig. 9.7




Axial PET and CT images show significantly increased FDG uptake at left paraaortic lymph node (arrow)
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
