May fragment and enter small bowel where they absorb water, increase in size, and become impacted
May present with small-bowel obstruction
• Drinking several liters of cola beverage has been reported to clear all or portions of phytobezoars
• Symptomatic, large phytobezoars or trichobezoars require endoscopic fragmentation or surgical removal
Spontaneous expulsion of bezoar is uncommon
(Left) Film from an upper GI series in a 60-year-old man with early satiety years after vagotomy and Billroth 1 surgery shows evidence of the prior surgery and a large heterogeneous “ball” of debris and gas within the stomach mixed with the barium.
(Right) Axial CECT shows a laminated mass in the stomach due to a phytobezoar.
(Left) Upper GI series in a 3-year-old girl with vomiting shows a fixed filling defect in the stomach with a swirled pattern of gas and solid material found to represent a trichobezoar.
(Right) A film from a small bowel follow-through shows evidence of a prior Billroth II partial gastrectomy and complete obstruction of antegrade flow of barium in the mid jejunum. At surgery, a phytobezoar was removed, which corresponded to the shape and size of the gastric remnant.
TERMINOLOGY
Definitions
• Intragastric mass composed of accumulated ingested (but not digested) material
IMAGING
General Features
• Best diagnostic clue
CT or fluoroscopy: Intraluminal mass containing mottled air pattern
• Location
Sites of impaction: Stomach, jejunum, ileum
– Narrowest portion of small bowel 50-75 cm from ileocecal valve or valve itself
– Any part can be affected, especially in patients with postoperative adhesions
• Morphology
Large bezoars fill and take shape of stomach
Radiographic Findings
• Radiography
Abdominal plain film: Soft tissue mass floating in stomach at air-fluid interface
– Mottled radiotransparencies in interstices of solid matter
– ± bowel obstruction
Insensitive test; bezoar identified in only 10-18% of patients from radiographs alone
Fluoroscopic Findings
• Intraluminal filling defect
With finely lobulated, villous-like surface
Freely mobile, without constant site of attachment to bowel wall
• Barium outlines bezoar
“Mottled” or streaked appearance; contrast medium entering interstices of bezoar
• Filling defect may occasionally appear completely smooth
Could be mistaken for enormous gas bubble that is freely movable within stomach
• Coiled spring appearance (rare)
• Partial or complete small bowel obstruction
Try to distinguish obstruction due to postoperative adhesions from bezoar-induced obstruction
CT Findings
• Well-defined, oval, low-density, intraluminal mass
“Mottled” appearance of mass is due to air bubbles retained in interstices of mass
Heterogeneous mass without postcontrast enhancement
– Pockets of gas, debris, fluid scattered throughout
– No air-fluid level within lesion
• Large bezoars tend to fill lumen
• Small bezoars are rounded or ovoid; tend to float on water-air surface surrounded by gastric contents
Oral contrast material may be seen surrounding mass, establishing free intraluminal location
• Bezoar may have “laminated” appearance
Ultrasonographic Findings
• Intraluminal mass with hyperechoic arc-like surface
With marked acoustic shadowing
• Identification of additional intestinal or gastric bezoars may be difficult
Only gold members can continue reading. Log In or Register to continue













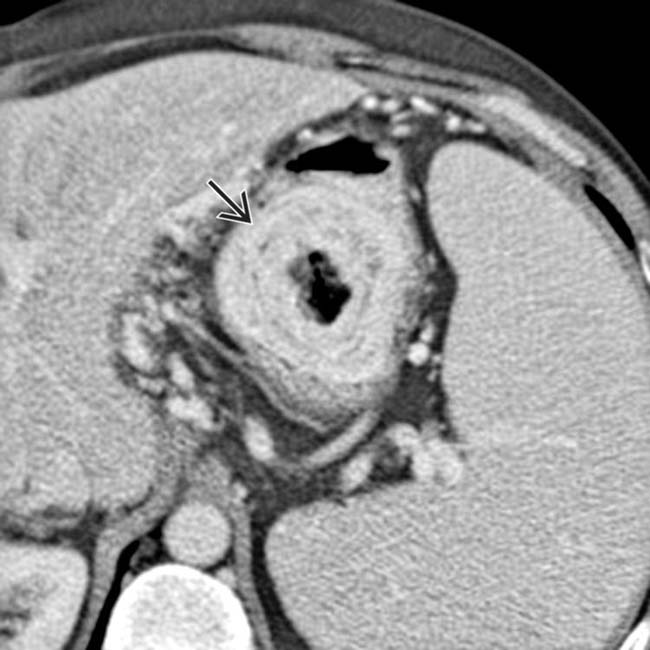
 in the stomach due to a phytobezoar.
in the stomach due to a phytobezoar.



















