Chapter 15 Gastric Carcinoma
Introduction
Over the past several decades, the incidence of gastric carcinoma in the world has been on a decline. But it remains the second most common cause of cancer-related death worldwide. There are differences in the geographic distribution, epidemiologic trends, presentation, and location of gastric carcinoma that have been studied in detail recently. Gastric carcinoma tends to be diagnosed at an advanced stage, particularly in the West, and generally has a poor prognosis. Japan has the highest incidence of gastric carcinoma, but it also has a national gastric carcinoma screening program, allowing for more patients being diagnosed at an early stage. For localized gastric carcinoma, the best chance for durable disease control and survival is with curative surgery. Unfortunately, surgery alone is not enough when the 5-year overall survival (OS) rate is 23% to 25%.1,2Multimodality therapy has become common practice for resectable gastric carcinoma to improve the rate of disease control and minimize recurrence. Postoperative chemoradiotherapy is the standard of practice in the United States and other parts of North and South America, and perioperative chemotherapy is adopted by most European countries. Regional differences of outcome are probably due to many different factors, most importantly, early disease detection in countries with a screening program, such as Japan, and also difficulty in accurate staging with currently available imaging and staging modalities.
Epidemiology and Risk Factors
Epidemiology
Although the incidence of gastric carcinoma is decreasing in Western countries, it remains the fourth most frequent cancer diagnosed and the second most lethal cancer worldwide, behind only lung cancer. The number of new cases of gastric carcinoma worldwide was recently estimated as over 600,000 in males and 330,000 in females.3 It is the third most common cancer in males and the fifth most common cancer in females worldwide.4 Sixty percent of cases occur in developing countries.5 The areas with the highest incidence rates are Eastern Asia, South America, and Eastern Europe. Regions in which gastric carcinoma is least frequent are North America, Western Europe, and parts of Africa. There is approximately a 20-fold difference in the incidence rates between Japan and some white populations in the United States.5 In the United States, approximately 21,520 new cases of gastric carcinoma were expected to be diagnosed during 2011, with 10,340 estimated deaths from the disease during the same period.6
Of the several classification systems that have been proposed to describe gastric carcinoma, the Lauren classification is the most widely used. The Lauren classification describes tumors based on the microscopic configuration and growth pattern into intestinal and diffuse types.7,8 Diffuse cancers are noncohesive and diffusely infiltrate the stomach. These often exhibit deep infiltration of the gastric wall and show little or no gland formation. These tumors are often associated with marked desmoplasia and inflammation with relative sparing of the overlying mucosa. The intestinal type, conversely, shows recognizable gland formation similar in microscopic appearance to the colonic mucosa. The glandular formation ranges from well- to poorly differentiated tumors and grows in expanding rather than infiltrative patterns.5 Intestinal cancers are believed to be related to environmental factors and are thought to arise secondary to chronic atrophic gastritis. The diffuse cancers, conversely, are less related to environmental factors and occur more often in young patients.5 The relative incidence of diffuse cancers is believed to have increased mainly owing to the decrease in the incidence of intestinal cancers.9
There are regional differences in the pathology and anatomic location of gastric carcinoma. A predominance of the Lauren intestinal type of adenocarcinoma occurs in high-risk areas, whereas the Lauren diffuse type is relatively more common in low-risk areas. Proximal gastric carcinomas and cancers of the gastroesophageal junction are more common in the West, and distal gastric carcinoma is more common in high-risk regions. At the M. D. Anderson Cancer Center, 41% of all UGI cancers involve the gastroesophageal junction.10 A steady decline in the incidence and mortality rates of gastric carcinoma has been observed worldwide over the past several decades. This is mainly due to a decrease in the intestinal variety of gastric carcinoma, the incidence of diffuse cancer being relatively stable.5
Etiology and Risk Factors
Because gastric carcinoma is more common in Asian than in Western countries, ethnic origin was thought to be an important contributory factor for the observed difference.11 Although first-generation Asian immigrants to Western countries carry the same high susceptibility for gastric carcinoma as their counterparts in their native country, subsequent generations acquire risk levels approaching that of the population of their adopted countries. This epidemiologic pattern underlines the importance of environmental factors in the pathogenesis of gastric carcinoma.12 Diets poor in fruits and vegetables and rich in smoked or poorly preserved food, salt, nitrates, and nitrites; infection with Helicobacter pylori; and smoking have all been currently implicated as significant risk factors in the development of gastric carcinoma in several studies.13–15 Chronic atrophic gastritis, previous gastric surgery, gastric polyps, and obesity, as well as low socioeconomic status, are also associated with an increased risk of gastric carcinoma.16,17
Gastric carcinoma is also seen as a part of the hereditary nonpolyposis colon cancer syndrome and other gastrointestinal (GI) polyposis syndromes such as Peutz-Jeghers syndrome and familial adenomatous polyposis.17 Mutations in the E-cadherin gene are a well-recognized cause of hereditary diffuse gastric cancer.18
Clinical Presentation
The symptoms of patients with gastric carcinoma are nonspecific. As a result, diagnosis is often delayed, and patients will have advanced disease at the time of diagnosis. Frequent symptoms associated with gastric carcinoma include dysphagia, early satiety, nausea, vomiting, and other symptoms attributable to gastric outlet obstruction or anemia. However, the most common symptoms at the time of diagnosis are upper abdominal pain and weight loss.19
Anatomy and Pathology
Anatomy
Being a derivative of the foregut, the stomach is almost entirely supplied by the branches of the celiac trunk (Figure 15-1). The left gastric artery, arising from the celiac axis, and the right gastric artery, a branch of the hepatic artery, supply the lesser curvature in the gastrohepatic ligament and form an anastomotic arcade along the lesser curvature. The left and right gastroepiploic arteries, branches of the splenic artery and the gastroduodenal artery, supply the greater curvature of the stomach and traverse the gastrosplenic ligament and the gastrocolic ligament, respectively. The gastrocolic ligament is the supracolic part of the greater omentum. Numerous short gastric arteries, branches of the splenic artery, also supply the greater curvature. A rich lymphatic network accompanies these vessels, creating a conduit for lymphatic drainage, and traverses these complex ligamentous structures. The various ligamentous attachments can be identified by noting vascular landmarks on cross-sectional imaging (Table 15-1).20 These ligamentous structures are important to understand because they represent the critical conduits for local extension of primary gastric carcinoma.
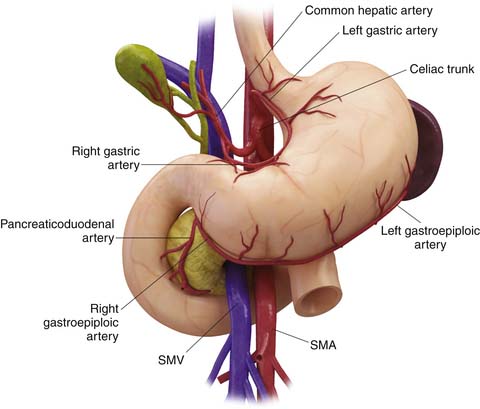
Table 15-1 The Various Ligamentous Attachments of the Stomach Can Be Identified by Identifying Vascular Landmarks on Cross-Sectional Imaging
| PERITONEAL LIGAMENTS AND FOLD | RELATION TO ORGANS | VASCULAR LANDMARK |
|---|---|---|
| Gastrohepatic ligament | Lesser curvature of the stomach to the liver | Left and right gastric arteries |
| Hepatoduodenal ligament | From the duodenum to the hepatic fissure | Proper hepatic artery, portal vein |
| Gastrocolic ligament | Greater curvature of the stomach to the transverse colon | Left and right gastroepiploic arteries and vein |
| Gastrosplenic ligament | From the left side of the greater curvature of the stomach to the splenic hilum | Left gastroepiploic vessels |
From Vikram R, et al. Pancreas: peritoneal reflections, ligamentous connections, and pathways of disease spread. Radiographics. 2009;29:e34.
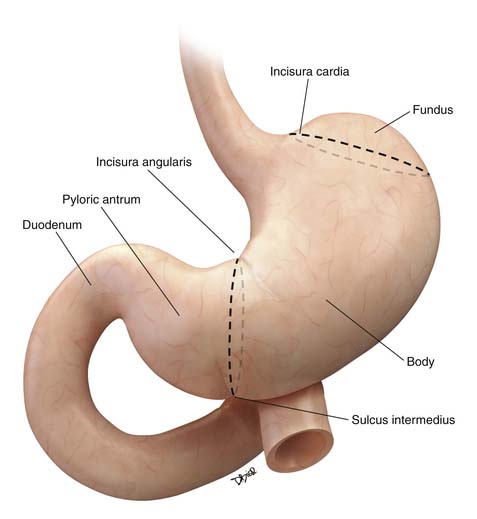
The stomach is divided for descriptive purposes into the fundus, body, pyloric antrum, and pylorus by imaginary lines drawn on its external surface (Figure 15-2). The fundus is dome-shaped, immediately under the left dome of the diaphragm, and is superior to the cardiac orifice. It lies above an imaginary line drawn horizontally at the level of the cardia (incisura cardia) to the greater curvature. At the lower end of the lesser curvature is a constant external notch (incisura angularis). The body extends from the cardia to the incisura angularis. A slight groove, the sulcus intermedius on the greater curvature of the stomach, separates the body from the pyloric antrum. The antrum extends from an imaginary line drawn from the incisura angularis to the sulcus intermedius. The pylorus is the narrowest part of the stomach, measuring only about 1 to 2 cm in length, and terminates into the duodenum (see Figure 15-2).21
Key Points Anatomy
• The stomach is divided into the fundus, body, pyloric antrum, and pylorus by imaginary lines drawn on its external surface.
• The stomach is almost entirely supplied by the branches of the celiac artery.
• Complex ligamentous attachments of the stomach provide conduits for direct spread of malignancies to the adjoining structures and the peritoneum.
Pathology
Malignant tumors of the stomach can be divided into four major subtypes based on cells of origin: epithelial, mesenchymal, and neuroendocrine tumors, and lymphoma. Leiomyosarcomas, neurofibrosarcomas, and malignant GI stromal tumors are mesenchymal in origin. The WHO classification of gastric tumors takes into consideration the morphologic and molecular characteristics of the tumors and is shown in Table 15-2.5
Table 15-2 The World Health Organization Classification of Tumors of the Stomach
| EPITHELIAL TUMORS | NONEPITHELIAL TUMORS |
|---|---|
| Intraepithelial neoplasia—adenoma | Leiomyoma |
| Carcinoma | Schwannoma |
| Adenocarcinoma | Granular cell tumor |
| Papillary adenocarcinoma | Glomus tumor |
| Tubular adenocarcinoma | Leiomyosarcoma |
| Mucinous adenocarcinoma | Gastrointestinal stromal tumor |
| Signet-ring cell carcinoma | Kaposi’s sarcoma |
| Adenosquamous carcinoma | |
| Squamous cell carcinoma | |
| Small cell carcinoma | |
| Undifferentiated carcinoma | |
| Carcinoid (well-differentiated endocrine neoplasm) |
Modified from Hamilton SR, Aaltonen LA, eds. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Digestive System. Lyon, France: IARC Press; 2000.
Malignant epithelial tumors constitute the majority of gastric neoplasias, and nearly 90% of them are adenocarcinomas. Several classification systems are used for describing adenocarcinomas. Based on histology, they are subdivided into tubular, papillary, mucinous, and signet-ring cell carcinomas.5 Usually, one of the subtypes predominates in adenocarcinomas. Based on gross appearance, it is classified into four types. Type I is a polypoid and fungating variety; type II is a polypoid tumor with central ulceration; type III is an ulcerated tumor with infiltrative margins; and type IV is linitis plastica.8,22 This method of classification is called the Borrmann classification and is generally reserved for advanced cancers. However, the simplest and the most widely accepted classification is the Lauren classification in which the gastric carcinomas are divided into two types: intestinal and diffuse.7,8 The intestinal type is associated with various degrees of glandular formation and intestinal metaplasia. The diffuse type is infiltrative and presents as a plaque or linitis plastica and tends to be poorly differentiated or of a signet-ring variety.5 Those cancers having features of both intestinal and diffuse types are considered mixed.
Key Points Pathology
• Ninety percent of malignant epithelial tumors of the stomach are adenocarcinomas.
• Several histologic classification systems are used, but the simplest and most widely accepted is the Lauren classification in which gastric carcinomas are divided into two types: intestinal and diffuse.
• Intestinal cancers show an expansile growth pattern with recognizable gland formation similar in microscopic appearance to the colonic mucosa. Diffuse cancers are noncohesive, diffusely infiltrate the gastric wall, and are associated with desmoplasia and inflammation.
Patterns of Tumor Spread
Gastric carcinoma shows a propensity to spread through direct contiguous invasion of adjacent peritoneal reflections and also to adjacent organs. In addition, dissemination via lymphatic and hematogenous routes also occurs. Both Lauren intestinal and diffuse varieties show a propensity for direct contiguous spread, but it is more commonly seen in the diffuse type of cancer. The gastrocolic, gastrohepatic, gastrosplenic, and hepatoduodenal ligaments all serve as conduits for tumor dissemination. Once the integrity of the peritoneal lining is breached, the tumor can seed into the peritoneal cavity, likely in the greater omentum, the paracolic gutters, and the pelvic floor. It is not uncommon to encounter tumor deposits in the ovaries and the rectovesicle pouch.
Periserosal implants into adjacent and distant organs are not infrequent, particularly with diffuse cancers, producing an appearance similar to linitis plastica, commonly in the colon.23,24
Lymphatic spread is seen commonly in advanced and not infrequently in early gastric carcinomas. Several nodal stations drain the stomach. These generally run parallel to the gastric blood supply: lymphatics along the lesser curve drain to the left gastric and celiac nodes; lymphatics along the pylorus and lesser curvature run parallel to the right gastric artery and drain into the hepatic and celiac nodes; a third group of lymphatics drain the proximal greater curvature of the stomach into the pancreaticosplenic nodes; and the fourth group parallels the right gastroepiploic vessels along the greater curvature and drain into the infrapyloric nodes and the nodes in the transverse mesocolon (Figure 15-3).
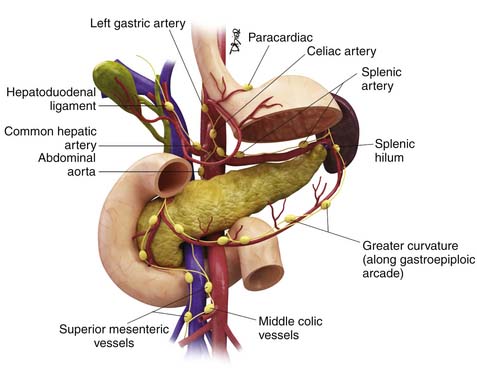
Figure 15-3 The major nodal stations draining the stomach. These generally parallel the gastric blood supply.
Key Points Pattern of tumor spread
• Direct contiguous spread occurs via the various ligamentous connections of the stomach such as the gastrocolic, gastrohepatic ligament, gastrosplenic, and hepatoduodenal ligaments.
• Peritoneal dissemination and seeding are common in advanced gastric carcinoma. Transperitoneal seeding of tumor to other abdominal organs is also seen.
• Lymphatic spread is to the perigastric and regional lymph nodes running parallel to the branches of the celiac artery.
• Hematogenous spread occurs to the liver, lungs, bones, and other soft tissues.
Staging
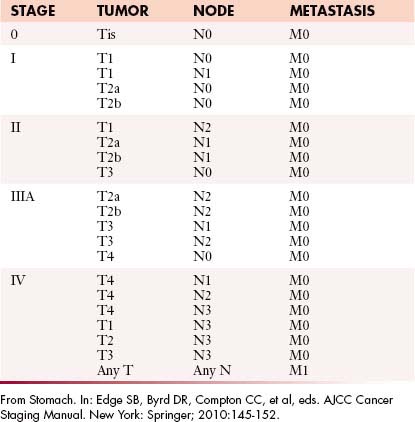
The tumor, node, and metastasis (TNM) staging is the most widely accepted method for staging gastric carcinomas.25 Radiologic investigations such as CT, MRI, and ultrasound (US) are used for preoperative staging. Pathologic staging is considered the gold standard, particularly in specimens not subject to preoperative chemo- or radiotherapy (Tables 15-3 and 15-4).
Table 15-3 The American Joint Committee on Cancer Tumor-Node-Metastasis Classification
| Primary Tumor (T) |
| TX: Primary tumor cannot be assessed |
| T0: No evidence of primary tumor |
| Tis: Carcinoma in situ: intraepithelial tumor without invasion of the lamina propria |
| T1: Tumor invades the lamina propria or submucosa |
| T2: Tumor invades the muscularis propria or the subserosa |
| T2a: Tumor invades the muscularis propria |
| T2b: Tumor invades the subserosa |
| T3: Tumor penetrates the serosa (visceral peritoneum) without invading adjacent structures |
| T4: Tumor invades adjacent structures |
| Regional Lymph Nodes (N) |
| NX: Regional lymph node(s) cannot be assessed |
| N0: No regional lymph node metastasis |
| N1: Metastasis in 1 to 6 regional lymph nodes |
| N2: Metastasis in 7 to 15 regional lymph nodes |
| N3: Metastasis in more than 15 regional lymph nodes |
| Distant Metastasis (M) |
| MX: Distant metastasis cannot be assessed |
| M0: No distant metastasis |
| M1: Distant metastasis |
From Stomach. In: Edge SB, Byrd DR, Compton CC, et al, eds. AJCC Cancer Staging Manual. New York: Springer; 2010:145-152.
Depth of invasion or T stage is an important independent prognostic factor for both survival and local recurrence. T1 cancers have a 10-year survival rate of approximately 80%, T2 lesions have a 10-year survival rate of 55%, and T3 and T4 lesions, only 30%.26–29
Knowledge of nodal anatomy is very important in staging lymph nodes in gastric carcinoma, because this is useful in surgical planning. The Japanese Research Society for Gastric Carcinoma has classified the regional lymph nodes based on location.30 These are further classified as compartments 1 to 4. Compartment 1 consists of the perigastric lymph nodes. Compartment 2 includes lymph nodes along the left gastric artery, common hepatic artery, celiac axis, and splenic artery. Compartment 3 includes lymph nodes along the hepatoduodenal ligament, at the posterior head of the pancreas, and at the root of the mesentery. In cancers of the antrum, the lymph nodes along the splenic artery are classified as compartment III. Para-aortic lymph nodes constitute compartment 4. These are useful in describing the extent of lymph node dissection in surgery. D1 dissection includes compartment 1; D2, compartments 1 and 2; D3 dissection compartments 1, 2, and 3; and D4 dissection includes all four compartments.
Although compartmental dissection is methodologically sound, the International Committee on Gastric Carcinoma has recommended that, for accurate staging and predicting prognosis, a minimum of 16 lymph nodes has to be included in the surgical specimen before an N stage can be determined.31 N stage is an independent variable for survival: N0 disease has a 10-year survival rate of 70%; N1, 41%; and N2 or N3, less than 20%.32
Key Points Staging
• TNM system is the most commonly used system and is an important prognostic factor.
• Nodal stations are classified into different compartments based on the distance from the primary tumor. These compartments are used to guide surgery.
• At least 16 nodes should be harvested at surgery and pathologically evaluated to complete pathologic staging for gastric carcinoma.
Imaging Evaluation
Tumor Detection and Staging
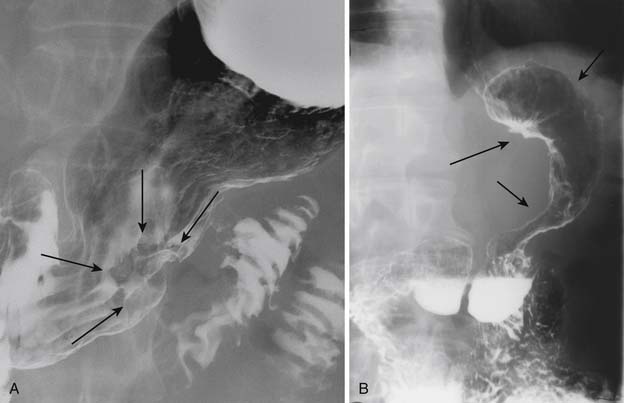
EGD has replaced UGI double-contrast barium study as the modality of choice to detect and diagnose gastric carcinoma owing to its specificity and the advantage of obtaining a tissue biopsy and also the ability to perform EUS, which offers a reliable way to T-stage the tumor.33 However, some reports indicate that endoscopy and UGI barium studies are equally sensitive in detection of primary gastric carcinoma.34,35 Gastric carcinoma has various appearances on GI barium studies. These include plaquelike lesions, sessile or pedunculated polypoid lesions, ulcerated lesions, and nondistention of the stomach as in the scirrhous type of carcinoma or linitis plastica with diffuse loss of mucosal detail (Figure 15-4).
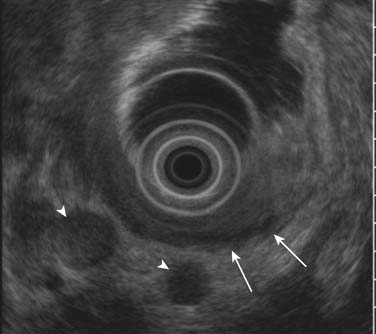
EUS is superior to all other modalities in visualizing the different layers of the gastric wall and, thus, is most accurate in preoperative local (T) staging of gastric tumors with a accuracy rate of 78% to 94%.36,37 Despite this, it is not uncommon (particularly for T2 tumors) that there is discordance with the actual pathologic specimen. The gastric wall layers appear as a five-layered structure on EUS with alternating hyperechoic and hypoechoic bands: serosa, muscularis propria, submucosa, deep mucosa, and superficial mucosa.38 Tumors generally are hypoechoic or hyperechoic and are seen disrupting this regular pattern. EUS is also valuable in assessing smaller perigastric lymph nodes (Figure 15-5). EUS is of little to no benefit after preoperative therapy.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


