Sharply defined mucosal defect (ulcer); smooth, even, radiating folds to edge of ulcer crater
Projects beyond expected contour of stomach (on upper GI and CT imaging)
Usually on lesser curve, posterior wall, or antrum
CT may show extravasation of gas and oral contrast (lesser sac or greater peritoneal cavity)
• Malignant ulcer
Uneven shape; irregular or asymmetric edges; interruption and clubbing of radiating folds
Does not project beyond contour of stomach
CT may show metastasis to nodes, peritoneum, liver
• Imaging for diagnosis
Upper GI series to show ulcer
CT to show complications (± ulcer itself)
CT gastroscopy in experienced hands may compete with endoscopy
• Sump ulcers: Distal 1/2 of greater curvature (NSAIDs)
• Incisura defect: Smooth or narrow indentation on curvature opposite ulcer (muscle contraction)
TOP DIFFERENTIAL DIAGNOSES
• Gastritis
• Gastric GIST
• Gastric metastases and lymphoma
• Artifactual
PATHOLOGY
• 2 major risk factors: H. pylori (60-80%) and NSAIDs (20%)
CLINICAL ISSUES
• Benign (95%), malignant (5%)
• Often multiple: 20-30% prevalence
• Complications: Hemorrhage, perforation, gastric outlet obstruction, and fistula
(Left) Graphic shows a gastric ulcer with smooth gastric folds radiating to the edge of the ulcer crater. Note the infolding of the gastric wall “pointing” toward the ulcer, known as the incisura sign.
(Right) Film from an upper GI series shows an ulcer niche projecting off the lesser curve of the antrum. Note the smooth gastric folds that radiate to the edge of the ulcer crater.
(Left) CECT of a perforated gastric ulcer shows thickening of the antral wall and submucosal edema , along with free intraperitoneal gas and ascites . The patient was taken to surgery where a perforated antral ulcer was oversewn along with an omental patch.
(Right) A subsequent upper GI series in the same patient shows a large prepyloric ulcer as a fixed outpouching of barium. The antrum and pylorus are distorted.
TERMINOLOGY
Abbreviations
• Gastric ulcer (GU)
Definitions
• Inflammatory erosion of gastric mucosa ± submucosal or deeper penetration
IMAGING
General Features
• Best diagnostic clue
Sharply marginated barium collection with folds radiating to edge of ulcer crater on upper GI series
• Location
Benign GU
– Most common on lesser curvature or posterior wall of antrum or body
– 3-11% on greater curvature, 1-7% on anterior wall
Malignant GU
– Usually on greater curvature
• Size
Most diagnosed ulcers are > 1 cm
Giant (> 3 cm) ulcers are usually benign but have increased risk of complications (e.g., perforation)
• Morphology
Same criteria are used for findings on upper GI series, CT virtual gastroscopy, and endoscopy
Benign GU
– Sharply defined mucosal defect (ulcer); smooth, even, radiating folds to edge of ulcer crater
– Ulcer projects beyond expected contour of stomach (on upper GI and CT imaging)
Malignant GU
– Uneven shape; irregular or asymmetric edges; interruption and clubbing of radiating folds
– Does not project beyond contour of stomach
Radiographic Findings
• Upper GI series
Benign GU, profile view
– Ulcer crater: Round or ovoid collections of barium
– Hampton line: Thin radiolucent line separating barium in gastric lumen from barium in crater
– Ulcer mound: Smooth, bilobed hemispheric mass projecting into lumen on both sides of ulcer; outer borders form obtuse, gently sloping angles with adjacent gastric wall (edema or inflammation)
– Ulcer collar: Radiolucent rim of edematous mucosa around ulcer
– Ulcer projecting beyond gastric wall
– Smooth, symmetric radiating folds to edge of ulcer crater
– Incisura defect: Smooth or narrow indentation on curvature opposite ulcer (muscle contraction)
– Enlarged areae gastricae in adjacent mucosa (edema or inflammation)
– Sump ulcers: Distal 1/2 of greater curvature (due to NSAIDs)
– Linear barium-coated ulcer: Decreases in depth with healing
– Splitting of 1 ulcer to 2 smaller collections (healing)
– Central pit or depression, radiating folds, or retraction of adjacent gastric wall (scarring)
– Hourglass stomach: Marked narrowing of body (scarring)
Benign gastric ulcer, en face view
– Ring shadow: Shallow ulcer on anterior or posterior wall (barium-coated rim and unfilled crater)
Malignant GU, profile
– Carman meniscus sign: Ulcer crater and radiolucent elevated border
– Does not project beyond expected gastric contour
– Discrete tumor mass forms acute angles
Malignant GU, en face view
– Irregular crater eccentrically located within tumor mass
– Focal nodularity, distortion, or obliteration of adjacent areae gastricae (tumor infiltration)
– Nodular, clubbed, fused, or amputated folds
CT Findings
• CECT (use water or water-soluble oral contrast, with oral gas granules to optimally distend stomach)
May visualize ulcer itself as outpouching
Only gold members can continue reading. Log In or Register to continue











 projecting off the lesser curve of the antrum. Note the smooth gastric folds that radiate to the edge of the ulcer crater.
projecting off the lesser curve of the antrum. Note the smooth gastric folds that radiate to the edge of the ulcer crater.
 , along with free intraperitoneal gas
, along with free intraperitoneal gas  and ascites
and ascites  . The patient was taken to surgery where a perforated antral ulcer was oversewn along with an omental patch.
. The patient was taken to surgery where a perforated antral ulcer was oversewn along with an omental patch.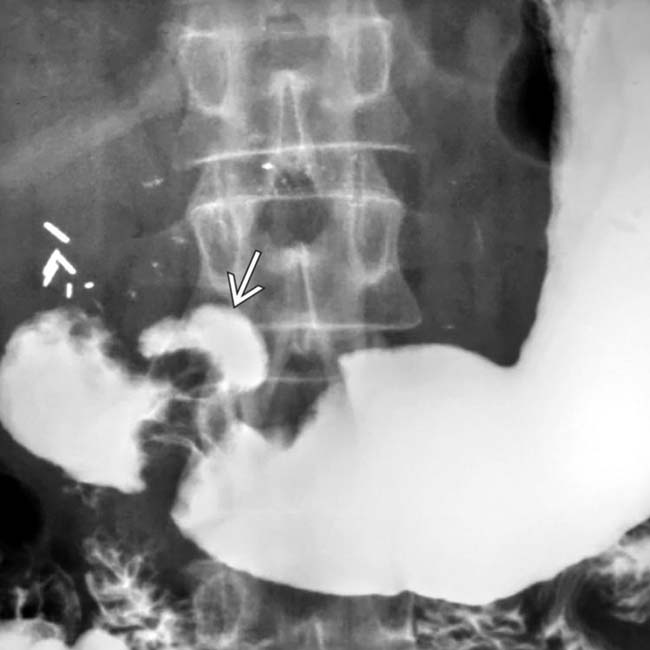
 as a fixed outpouching of barium. The antrum and pylorus are distorted.
as a fixed outpouching of barium. The antrum and pylorus are distorted.

















