High-density intramural hematoma, pneumoperitoneum, anterior pararenal space fluid/air
• Upper GI findings
Duodenal lumen narrowing by hematoma; contrast extravasation (peritoneal cavity, retroperitoneum)
• Best imaging tool: CECT, upper GI
TOP DIFFERENTIAL DIAGNOSES
• Perforated duodenal ulcer
• Villous adenoma
• Duodenal lymphoma
CLINICAL ISSUES
• Clinical profile
Child with midepigastric blunt trauma, adult with high-speed motor vehicle crash injuries
Other forms of blunt trauma (e.g., assault, sports injuries)
Iatrogenic injuries include endoscopy, especially with endoscopic sphincterotomy/papillotomy and stone removal from common duct
• Most common signs/symptoms
Nausea, vomiting, abdominal pain/tenderness
• Treatment
Nonoperative management for isolated hematoma without perforation
Surgery for duodenal perforation and head of pancreas injury (pancreaticoduodenal resection;modified Whipple)
DIAGNOSTIC CHECKLIST
• Consider perforated duodenal ulcer
• Clinical features are usually distinctive
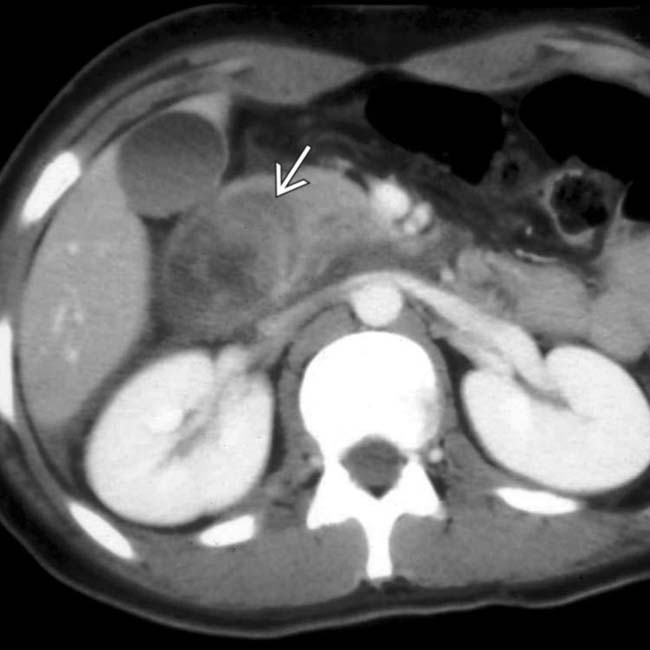
(Left) Axial CECT in a 16-year-old boy with blunt abdominal trauma shows a high-attenuation mass within the duodenal wall (hematoma) that narrows the duodenal lumen.
(Right) Another CT section in the same case shows the intramural hematoma extending into and narrowing the lumen of the 3rd portion of duodenum. This resulted in partial gastric outlet obstruction but resolved over the next 10 days with nonoperative management.
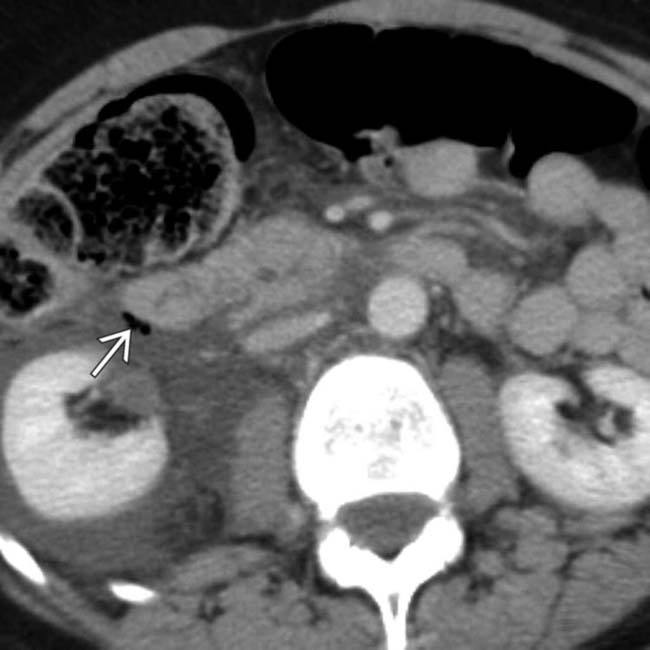
(Left) CT in a 25-year-old man had blunt trauma shows extensive fluid &/or infiltration of the anterior pararenal and perirenal spaces. Signs of pancreatic injury include indistinct appearance of the pancreatic head, a thin fracture plane through the neck , and fluid between the pancreas and the splenic vein .
(Right) Another CT section in the same patient shows gas bubbles adjacent to the duodenum indicating duodenal perforation (confirmed at surgery) along with pancreatic transection.
TERMINOLOGY
Definitions
• Trauma to duodenum resulting in intramural hematoma or laceration







 within the duodenal wall (hematoma) that narrows the duodenal lumen.
within the duodenal wall (hematoma) that narrows the duodenal lumen.
 extending into and narrowing the lumen of the 3rd portion of duodenum. This resulted in partial gastric outlet obstruction but resolved over the next 10 days with nonoperative management.
extending into and narrowing the lumen of the 3rd portion of duodenum. This resulted in partial gastric outlet obstruction but resolved over the next 10 days with nonoperative management.
 spaces. Signs of pancreatic injury include indistinct appearance of the pancreatic head, a thin fracture plane through the neck
spaces. Signs of pancreatic injury include indistinct appearance of the pancreatic head, a thin fracture plane through the neck  , and fluid between the pancreas and the splenic vein
, and fluid between the pancreas and the splenic vein  .
.
 adjacent to the duodenum indicating duodenal perforation (confirmed at surgery) along with pancreatic transection.
adjacent to the duodenum indicating duodenal perforation (confirmed at surgery) along with pancreatic transection.









