Figure 10.1.1
Esophageal atresia. There is severe polyhydramnios and no identifiable stomach on this transverse view of the fetal upper abdomen.
10.2. Duodenal Atresia
Description and Clinical Features
Duodenal atresia is a disorder in which the duodenum is obstructed by a segment that has complete obliteration of the lumen. The atretic segment is usually just distal to the duodenal bulb, in the second portion of the duodenum.
Duodenal atresia may occur as an isolated anomaly or in association with other anomalies. Approximately one-third of fetuses with duodenal atresia have trisomy 21.
Duodenal atresia is the most common, but not the only, cause of duodenal obstruction. Other causes include annular pancreas, intestinal malrotation with Ladd’s bands, and duodenal web.
Sonography
Sonographic diagnosis of duodenal obstruction is made when two findings are present: (1) dilation of the fetal stomach and duodenum (“double bubble”), appearing sonographically as two prominent fluid-filled structures in the upper abdomen and (2) polyhydramnios (Figure 10.2.1). On a coronal or oblique view of the fetal abdomen, the dilated stomach and duodenum can sometimes be seen to be connected to one another (Figure 10.2.2). The specific diagnosis of duodenal atresia can be suspected, but not established with certainty, because other causes of duodenal obstruction have similar sonographic findings (Figure 10.2.3).

Figure 10.2.1
Duodenal atresia, with “double bubble”, in a fetus with trisomy 21. Transverse view of the fetal upper abdomen demonstrates two fluid-filled structures (“double bubble”), representing the dilated stomach (long arrow) and duodenum (short arrow). Amniotic fluid volume is high. Amniocentesis was performed and revealed trisomy 21.
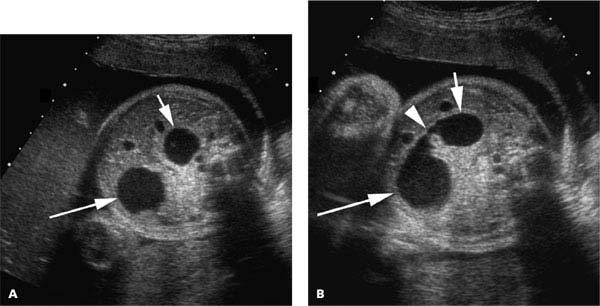
Figure 10.2.2
Duodenal atresia, with identifiable connection between stomach and duodenum, in a fetus with trisomy 21. A: Transverse view of the fetal upper abdomen demonstrates dilated stomach (long arrow) and duodenum (short arrow). B: Image in a slightly different plane demonstrates the connection (arrowhead) between the stomach (long arrow) and duodenum (short arrow). Amniocentesis was performed and revealed trisomy 21.
Because duodenal atresia is the most common cause of duodenal obstruction and is often associated with other structural or chromosomal anomalies, the entire fetus should be carefully examined whenever duodenal obstruction is suspected (i.e., whenever there is a “double bubble” and polyhydramnios). The parents should also be counseled that the fetus is at substantially increased risk of trisomy 21.

Figure 10.2.3
Duodenal obstruction due to annular pancreas. The stomach (long arrow) and duodenum (short arrow) are distended, and there is polyhydramnios. The baby died shortly after birth and an annular pancreas was found at autopsy.
10.3. Small Bowel Obstruction
Description and Clinical Features
Small bowel obstruction can occur at any point (or points) along the small bowel, from the proximal jejunum to the distal ileum. It can result from a number of causes, including atresia, volvulus, and a meconium plug. The latter cause is typically seen in fetuses with cystic fibrosis.
Because amniotic fluid is consumed by fetal swallowing and small bowel absorption, the amniotic fluid volume is usually increased when the fetus has a small bowel obstruction. In general, the more proximal the obstruction is, the more severe the polyhydramnios.
Sonography
The sonographic findings of a small bowel obstruction depend on the level of obstruction but typically include dilated fluid-filled loops of bowel and polyhydramnios. With proximal jejunal obstruction, the sonogram shows a short segment of dilated bowel and moderate-to-severe polyhydramnios (Figure 10.3.1). With a distal ileal obstruction, there will be multiple loops of dilated bowel, and the amniotic fluid volume may be normal or mildly elevated (Figure 10.3.2).

Figure 10.3.1
Jejunal atresia. A: Transverse view through the fetal abdomen reveals a dilated segment of bowel (arrows). B: There is moderate-to-severe polyhydramnios.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


