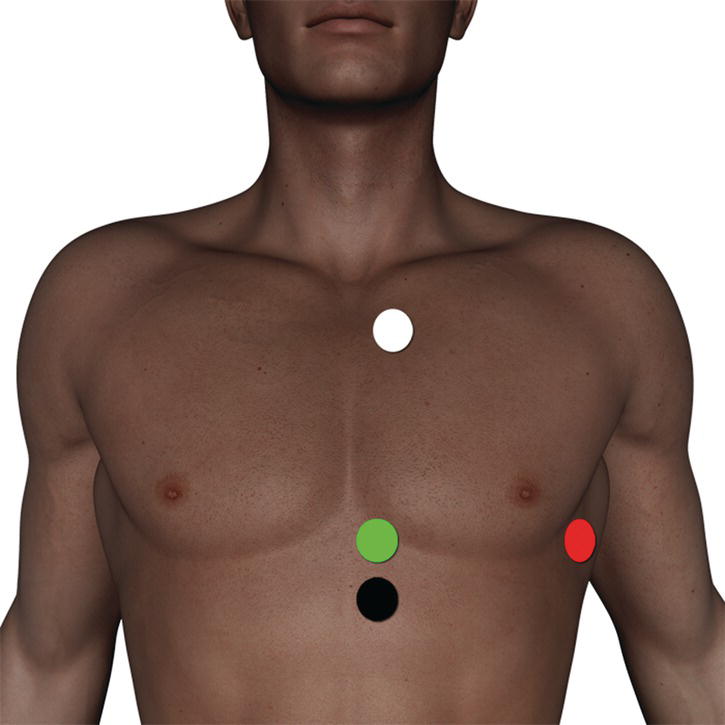
5 This section refers to the mechanisms and correct placement of gating leads and respiratory bellows. The basic concepts of these techniques are summarized in the following. Only a brief overview is provided here. For a more detailed explanation, please refer to Chapter 8 of MRI in Practice or an equivalent text. Cardiac gating uses the electrical signal detected by leads placed on to the patient’s chest to trigger each RF excitation pulse. In this way, each image is always acquired at the same phase of the cardiac cycle, so that phase mismapping from cardiac motion is reduced. There are several factors to take into account when using cardiac gating. There are usually four leads that are colour-coded for easy use. Some systems may only use three leads. In addition, not all systems use the same colour coding, but the principle of their placement is the same. Leads can be placed either anteriorly on the chest or posteriorly on the patient’s back. Anterior placement is usually simpler as the landmarks are easier to find. In addition, if the leads are placed posteriorly, the patient lies on them during the examination, which may be uncomfortable. The anterior lead placement is described here, but if the trace on the ECG monitor is poor, the leads can be placed posteriorly in a mirror image to the anterior leads. This may improve the trace. Lay the patient supine on the examination couch. The patient wears a front opening gown for easy access. The lead stickers are then firmly attached to the patient’s skin. The leads are usually colour-coded thus: The white and the red leads are placed across the heart, as the voltage difference between the two produces the ECG trace. The green and black leads (that act as grounds) are positioned as close as possible to each other, but not touching, in the centre of the chest. Some systems may not have colour coding, but directions on lead placement are usually given by the manufacturer. Leads can be placed in a variety of ways as long as the above criteria are met. Described below is the simplest method of lead attachment (Figure 5.1): Figure 5.1 The correct placement of gating leads. The black lead may be omitted if it is not available on the system. Once the leads are attached and plugged into the system, check that the ECG trace is satisfactory. Traces vary according to rate, rhythm and cardiac output. These in turn depend on the activity of the heart, which is often altered by certain disease processes. Arrhythmias and poor cardiac output (which may be why the patient is being examined) are common problems. The signs of a good trace are: Figure 5.2 A normal ECG Trace and the correct placement of the triggering threshold relative to the R wave. If the trace is satisfactory, the patient is placed within the magnet bore. This action frequently alters the trace, and often does so to such an extent that the trace is no longer acceptable. The commonest problem is an elevation of the T wave so that the system cannot distinguish it from the R wave. If this occurs, or if the original trace is unsatisfactory, several measures can be taken.
Gating and respiratory compensation techniques
Introduction
Cardiac gating (ECG gating)
Lead placement
How to improve the trace
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


