and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
14.1 Case 1: Restaging of Uterine Carcinosarcoma
History
A 62-year-old female who is status post total hysterectomy and bilateral salphyngoopherectomy had the diagnosis of malignant mixed Müllerian tumor and is now being evaluated for restaging with 18F-FDG PET/CT.
Findings
Fig. 14.1
Axial PET and CT images (a, b) show pelvic mass lesion with intense FDG uptake (SUVmax 16.6) and hypermetabolic lymph nodes at bilateral internal iliac region. There are lymph nodes at paraaortic, paracaval, and interaortocaval areas showing increased FDG uptake (SUVmax 6.6) (c, d). FDG accumulation at anterior wall of pelvis consistent with postoperative inflammation is also noticed
Fig. 14.2
MIP image (a), axial PET, CT, and fusion images (b–d) show hypermetabolic lymph nodes at paraaortic and paracaval areas
Interpretation
Local residual malignant tissue at pelvis and lymph nodes at among both iliac lymphatic chain showing metastatic involvement.
Teaching Point
Carcinosarcomas (malignant mixed Müllerian tumors) are rarely encountered malignancies, representing less than 5 % of all uterine tumors. 18F-FDG PET/CT has shown 87.5 % sensitivity of and 97.5 % specificity for detecting disease in asymptomatic patients, and 92.9 % and 100 %, respectively, for patients suspected of recurrence on CT.
14.2 Case 2: Restaging of Uterine Carcinosarcoma
History
A 51-year-old female who had undergone total hysterectomy and bilateral salphyngoopherectomy was being followed up with the diagnosis of malignant mixed Müllerian tumor. Patient received chemotherapy following the operation. Seven months after the operation 18F-FDG PET/CT scan is performed for restaging.
Findings
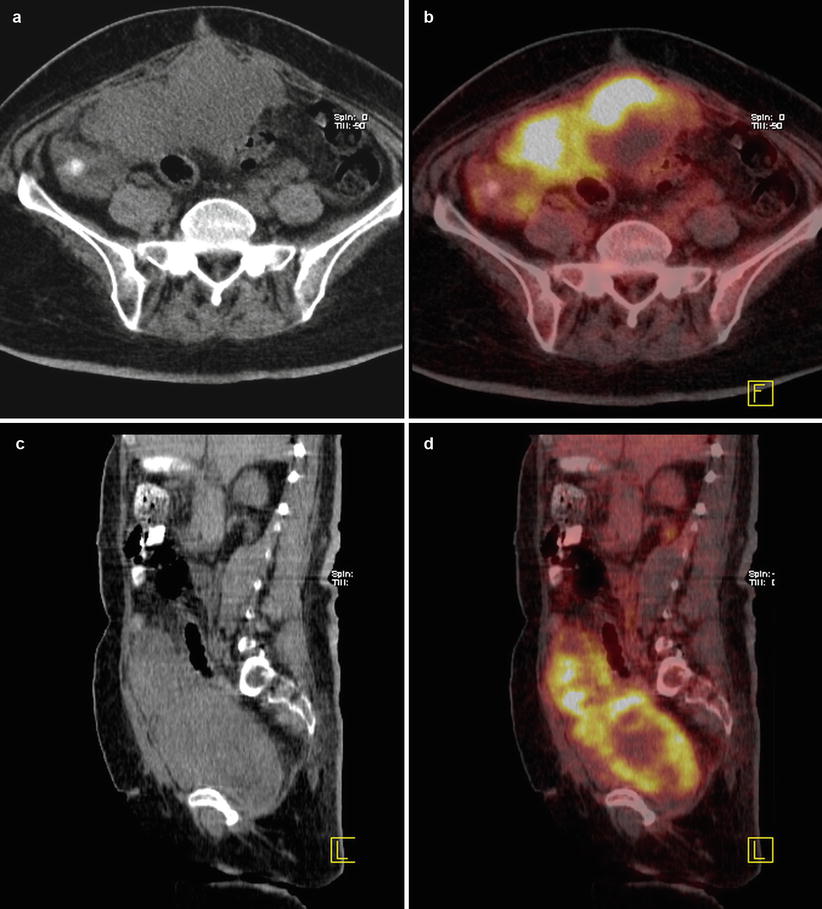
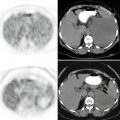
Fig. 14.3
Axial (a, b) and sagittal (c, d) CT and fusion images show intensely hypermetabolic (SUVmax 15.3) mass lesion with centrally necrotic hypometabolic areas. The lesion invades peritoneal surfaces and omental fat tissue
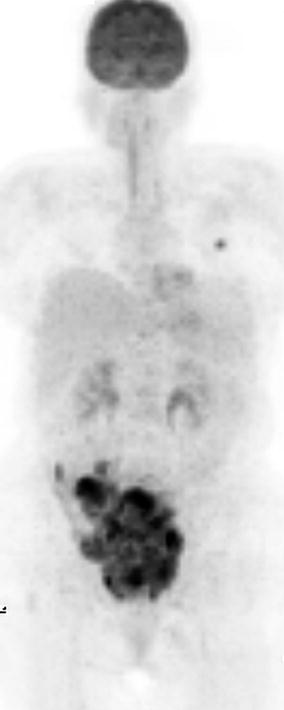
Fig. 14.4
MIP image
Interpretation
There is local recurrence and rapid progression of malignancy despite therapy which indicates bad prognosis.
Teaching Point
FDG PET/CT scan is effective in evaluating therapy response and predicting the prognosis in uterine sarcomas.
14.3 Case 3: Restaging of Uterine Endometrioid Adenocarcinoma
History
A 68-year-old female who is status post total hysterectomy, bilateral salphyngoopherectomy, and pelvic lymphadenectomy had the diagnosis of endometrioid adenocarcinoma and underwent 18F-FDG PET/CT scan for restaging.
Findings
Fig. 14.5
Axial CT and fusion images (a, b) show lymph node at left internal iliac area with extensive FDG uptake (SUVmax 13). Swelling at left lower extremity with mild diffuse increased FDG uptake is compatible with lymphedema (c, d)
Fig. 14.6
MIP image (a) show hypermetabolic lymph node at left pelvic region, and swelling at left lower extremity (b)
Interpretation
Lower limb lymphedema is caused by pelvic lymph node dissection. There is still left pelvic lymph node with metastatic involvement.
Teaching Point
Lymphedema occurs as a result of an obstruction or interruption of the lymphatic system, generally in proximal limb segments at lymph nodes, due to surgery, infection, malignancy, or scar tissue. Obstruction is frequently seen at pelvic and inguinal groups of nodes in the lower limbs.
14.4 Case 4: Ovarian Papillary Serous Adenocarcinoma
History
A 78-year-old female patient had ovarian papillary serous adenocarcinoma (PSAC) and had undergone total abdominal hysterectomy and bilateral salpingoophorectomy 2 years ago. Histopathology revealed PSAC with psammoma bodies within papillary tumor cells. Her CA 125 cerum level was 110.9 units (normal 0–35 units) and a calcified lesion at 6th segment of liver suspicious for metastasis was detected on CT. The patient was referred to us for further evaluation with 18F-FDG PET/CT.
Findings
Fig. 14.7
Axial CT and fusion images show calcified lesion at right upper paratracheal and paracardiac regions that exhibit moderate FDG uptake
Fig. 14.8
Axial PET and CT images show hypermetabolic calcified lesions at right anterior diaphragmatic area and adjacent to right lobe of liver
Fig. 14.9
Axial CT and fusion images show hypermetabolic calcified lesions at mesenteric fatty tissues
Fig. 14.10
Axial PET, CT, and fusion images show hypermetabolic calcified lesion at subcutaneous fatty tissues

Fig. 14.11
MIP image
Interpretation
Hypermetabolic calcified lesions consistent with metastases of ovarian PSAC.
Teaching point
PSAC accounts for approximately 40 % of all cancers of the ovary and are the most common malignant ovarian tumor. Extensive calcification of PSAC is due to high content of nearly spherical, concentrically laminated psammoma bodies.
14.5 Case 5: Therapy Response Evaluation in Ovary Carcinoma
History
A 68-year-old female status post hysterectomy and bilateral salpingoophorectomy for ovarian cancer underwent 18F-FDG PET/CT and metastatic lesions were detected. Two months after chemotherapy a control PET/CT scan was performed.
Findings
Fig. 14.12
Axial CT and PET images before (a, b) and after chemotherapy (c, d) showed focal intense FDG uptake at left upper quadrant of abdomen (SUVmax 8.6) and clearance of activity after chemotherapy
Fig. 14.13
Axial PET and CT images before (a, b) and after chemotherapy (c, d) show focal intense FDG uptake at left obturator region (SUVmax 7.5) and clearance of activity after chemotherapy
Fig. 14.14




Axial PET and CT images before (a, b) and after chemotherapy (c, d) show focal intense FDG uptake at right lower paratracheal region (SUVmax 7.8) and decrease in intensity of activity after chemotherapy (SUVmax 6)
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
