Figure 5.1
Endocavitary transducer position for tonsillar ultrasound: The endocavitary probe should be inserted to view the affected tonsil. It can help to have the patient direct you as they will be more comfortable this way

Figure 5.2
Carotid artery posterior to tonsil: The carotid artery (B) can be visualized posterior to the tonsil. A peritonsillar abscess can be seen in this image (A)

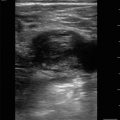
Figure 5.3
Peritonsillar abscess: A large area of hypoechoic fluid (arrow) represents a peritonsillar abscess

Figure 5.4
Needle with plastic cap cut: To avoid entering too far into the peritonsillar space, a needle cap can be cut to only allow a set amount of needle to enter
Thyroid Ultrasound
- (a)
- (b)
Thyroid Anatomy
A superficial endocrine organ in the neck that overlies the trachea.
The isthmus of the thyroid is the connection between the right and left lobes and usually lies over the second or third tracheal ring.
Each lobe is located anterior and lateral to the trachea, with the carotid artery and internal jugular veins located posteriorly.
- (c)
Transducer Selection
Linear array transducer
- (d)
Patient Position
The patient should be supine or in a semi-recumbent position with their neck extended.
- (e)
Standard Exam Views
Begin by imaging the thyroid gland in a transverse plane.
Place the transducer below the laryngeal prominence with the marker pointed toward the patient’s right.
Figure 5.5—Transducer position
Scan inferiorly until the isthmus of the thyroid is visualized.
Move the transducer laterally to each side to image the right and left lobes of the thyroid.
Figure 5.7—Thyroid lobes.
Lateral to each lobe will be the paired thick-walled anechoic and pulsatile carotid artery followed by the thinner-walled internal jugular vein [4].
The esophagus is often found posterior to the left thyroid lobe and anterior to the cervical vertebral body [3].
Visualized as an oval or flattened structure with alternating hypo- and hyperechogenicity [3].
Figure 5.8—Thyroid and surrounding structures.
Video 5.3—Thyroid ultrasound.
Rotate the transducer clockwise 90° with the marker pointed cephalad. Image each lobe of the thyroid in a sagittal plane.
Figure 5.9—Thyroid in a sagittal plane
Video 5.4—Thyroid in sagittal plane
Apply color Doppler to each area of the thyroid to evaluate vascular flow.
Figure 5.10—Color Doppler of the thyroid gland
Video 5.5—Color Doppler of the thyroid gland
- (f)
Thyroid Pathology
Thyroid nodule
Lesion within the thyroid gland caused by an overgrowth of thyroid cells.
Majority of thyroid nodules are benign with only about 5% malignant [5].
Common incidental findings on computed tomography or with ultrasound of the thyroid.
Will appear as a discrete lesion that distorts the normal thyroid echotexture [4].
Figure 5.11—Thyroid nodule.
Thyroid Cyst
A type of benign thyroid nodule.
Can be simple, colloid, or hemorrhagic
Simple cysts will appear as round, anechoic, or hypoechoic structures with posterior acoustic enhancement.
Figure 5.12—Thyroid cyst.
Video 5.6—Thyroid cyst.

Figure 5.5
Transducer position on neck: For thyroid ultrasound, having the patient sit in a supine position slightly recumbent can facilitate easy scanning of the neck

Figure 5.6
Isthmus of thyroid: The isthmus of the thyroid (arrow) will be seen anterior to the hyperechoic trachea

Figure 5.7
Thyroid lobes: Right (A) and left (B) thyroid lobes

Figure 5.8
Thyroid with surrounding structures: Lateral to each thyroid lobe will be the paired thick-walled anechoic and pulsatile carotid arteries (B) followed by the thinner-walled internal jugular veins (A). The esophagus (arrow) is often found posterior to the left thyroid lobe and anterior to the cervical vertebral body

Figure 5.9
Thyroid in a sagittal plane: Left lobe of the thyroid visualized in sagittal plane

Figure 5.10
Color Doppler of the thyroid gland: Normal vascular flow of the thyroid gland using color Doppler

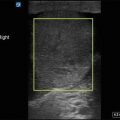
Figure 5.11
Thyroid nodule: A thyroid nodule (arrow) is a distinct lesion within the thyroid that is formed by an overgrowth of thyroid cells

Figure 5.12




Thyroid cyst: Thyroid cysts (arrow) are a type of benign nodule that can be simple, colloid, or hemorrhagic
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
