Intrahepatic or subcapsular fluid collection (hematoma) on US or CT
• CT not ideal due to radiation dose, but may be necessary in severe cases
• US: Irregular or wedge-shaped liver hemorrhage or infarct with increased echogenicity; usually peripheral
TOP DIFFERENTIAL DIAGNOSES
• Acute fatty liver of pregnancy
• Hepatic trauma
• Spontaneous hemorrhage (coagulopathy)
• Bleeding hepatic tumor (adenoma or HCC)
CLINICAL ISSUES
• Acute epigastric and RUQ pain
90% of cases
• 1-2 per 1,000 live births; 10-20% of eclamptic patients
• Clinical profile
African American female, primigravida, features of preeclampsia and lab data positive for hemolysis, elevated liver enzymes, and low platelets
• Classic triad of preeclampsia
Hypertension, proteinuria, edema
DIAGNOSTIC CHECKLIST
• In hypotensive patient, look for and embolize active bleeding
• Rarely can occur without classic preeclampsia triad
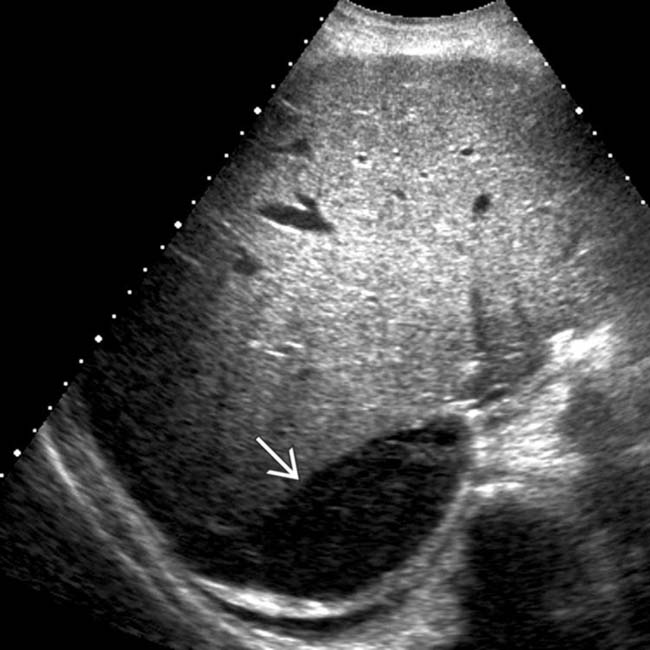
(Left) This is a transverse grayscale ultrasound image of a 39-year-old woman who presented with sharp RUQ and right pleuritic pain during her 3rd trimester of pregnancy. Laboratory values revealed markedly decreased platelets, consistent with HELLP syndrome. Note the mass effect on the liver from a predominantly hypoechoic subcapsular hematoma .
(Right) Longitudinal grayscale ultrasound image obtained in the same patient again shows the peripheral subcapsular hematoma .
(Left) This 35-year-old woman had toxemia and sudden RUQ pain with falling hematocrit. Axial CECT shows a massive subcapsular and perihepatic hematoma along with active bleeding and heterogeneous enhancement of the hepatic parenchyma .
(Right) A selective hepatic arteriogram shows multiple foci of active hemorrhage , which were treated with coil embolization. Following the birth of twins shortly after the angiogram, the patient made a complete recovery.
TERMINOLOGY
Abbreviations
• H emolysis, e levated l iver enzymes, l ow p latelets (HELLP)
Definitions
• Severe variant of preeclampsia
IMAGING
General Features
• Best diagnostic clue
Intrahepatic or subcapsular fluid collection (hematoma) on US, CT, or MR
CT Findings
• Liver hematomas
Well-defined, hyper- or hypodense, depending on physical state of blood
Nonenhancing
Acute: Hyperattenuating clot (24-72 hours)
Chronic: Decreased attenuation after 72 hours (lysed clot)
• Liver infarction
Small or large areas of low attenuation, usually peripheral and wedge shaped
May be indistinguishable from steatosis of pregnancy
• Occasionally active contrast extravasation or ascites
Active bleeding is serious; may require embolization or surgery
MR Findings
• Hemorrhage and necrosis (often coexist)
T1WI and T2WI
– T1WI: Low signal intensity
– T2WI: High signal intensity
– Varied signal intensity based on
Degree and age of hemorrhage, infarct, or steatosis
Greater degree of edema and cellular necrosis in infarction
Ultrasonographic Findings
• Grayscale ultrasound
Irregular or wedge-shaped liver hemorrhage or infarct with increased echogenicity; usually peripheral
Periportal halo sign: Hyperechoic thickening of periportal area




 .
.
 .
.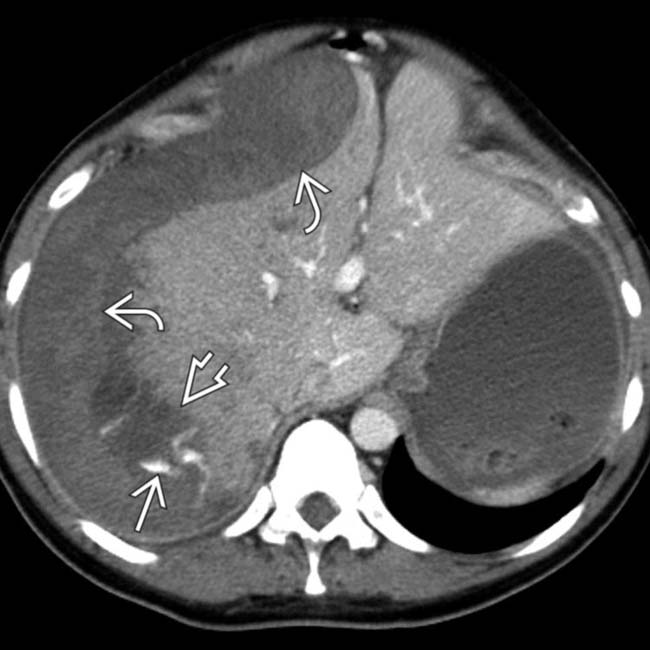
 along with active bleeding
along with active bleeding  and heterogeneous enhancement of the hepatic parenchyma
and heterogeneous enhancement of the hepatic parenchyma  .
.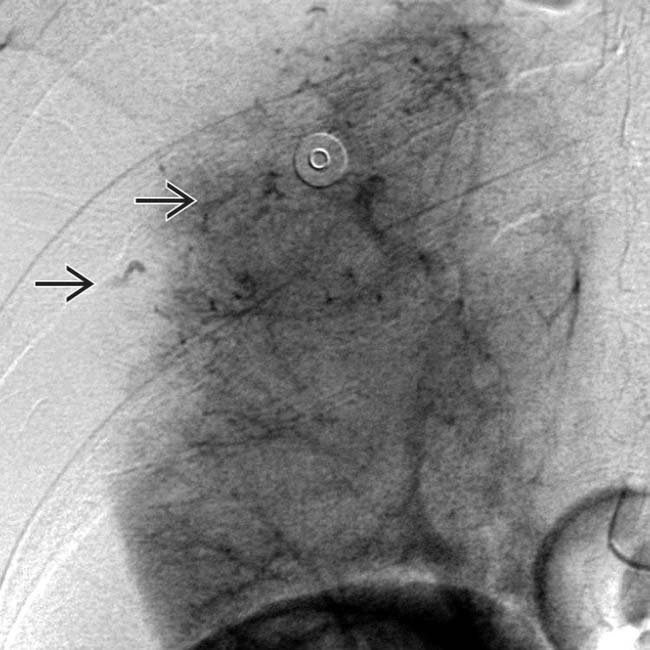
 , which were treated with coil embolization. Following the birth of twins shortly after the angiogram, the patient made a complete recovery.
, which were treated with coil embolization. Following the birth of twins shortly after the angiogram, the patient made a complete recovery.






















