Injury to bare area of liver may result in retroperitoneal, not intraperitoneal, bleeding
• Best imaging tool: MDCT in hemodynamically stable patients
• CT protocol advice: Rapid bolus of contrast; include lung bases and pelvis
• Angiography to localize active hemorrhage and embolization to control it
TOP DIFFERENTIAL DIAGNOSES
• HELLP syndrome
• Spontaneous hemorrhage (coagulopathy)
• Bleeding hepatic tumor (e.g., hepatocellular carcinoma or adenoma)
PATHOLOGY
• Blunt trauma is most common cause of hepatic injury
CLINICAL ISSUES
• Clinical profile: Patient with history of motor vehicle accident, right upper quadrant tenderness, guarding, and hypotension
• Mortality: 10-20%
• Liver is 2nd most frequently injured solid intraabdominal organ after spleen
DIAGNOSTIC CHECKLIST
• CT evidence of active extravasation
Intra- or extrahepatic collection, i sodense with vessels
Usually indicates need for embolization or surgery, regardless of grade of injury
• Laceration of left hepatic lobe is often associated with bowel and pancreatic injury
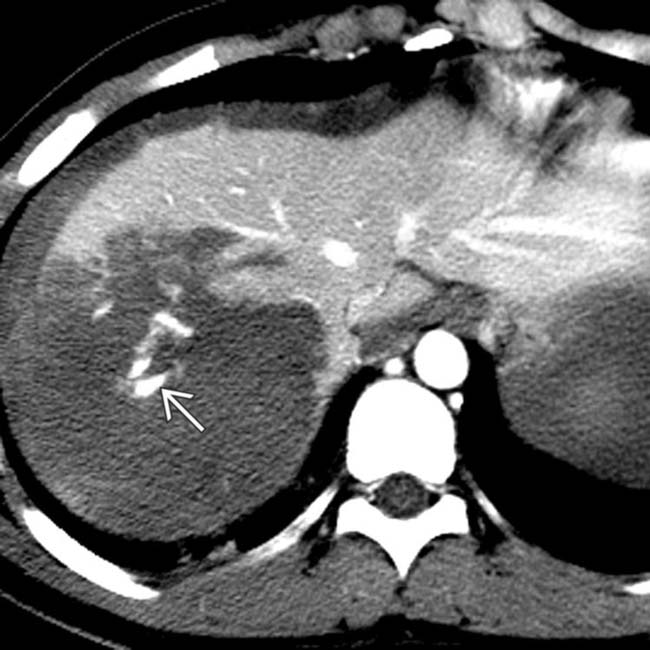
(Left) CT in a 37-year-old man who sustained blunt abdominal trauma in a motor vehicle accident shows a large right lobe hepatic injury (laceration & infarct or parenchymal hematoma) with high-attenuation active arterial extravasation .
(Right) Selective right hepatic artery angiogram in the same patient confirms active bleeding , which was successfully treated with a coil embolization. The patient made an uneventful recovery without the need for a blood transfusion.
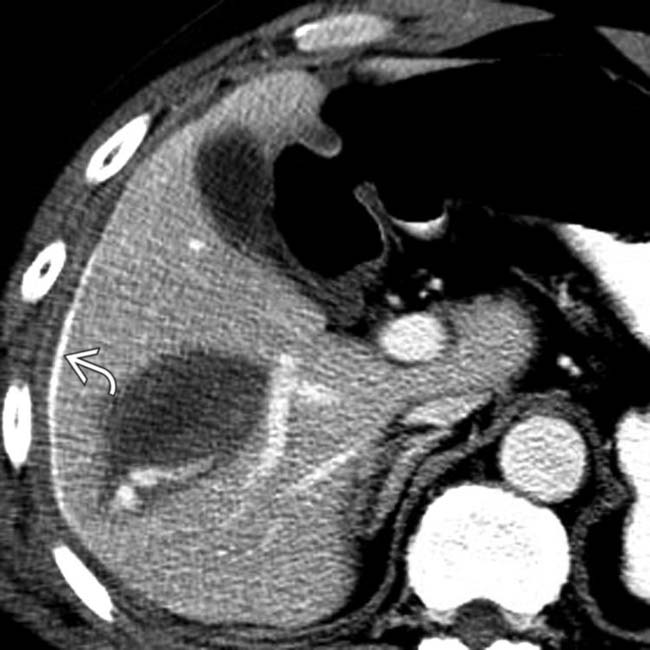
(Left) Axial CECT obtained in a 19-year-old man who sustained multiple injuries after a motorcycle accident demonstrates a right lobe hepatic laceration with active bleeding .
(Right) Axial CECT in the same patient shows extension of active bleeding into the peritoneal cavity along the hepatic capsule. Due to the acute intraperitoneal bleeding, urgent surgery was performed, which revealed an actively bleeding capsular artery.
TERMINOLOGY
Definitions
• Liver or hepatic injury
IMAGING
General Features
• Best diagnostic clue
CT evidence of irregular parenchymal lesions with intra- and perihepatic hemorrhage
• Location
Right lobe (75%), left lobe (25%)
– Intraparenchymal &/or subcapsular hematoma
CT Findings
• Lacerations: Simple or stellate (often parallel to portal/hepatic vein branches)
Simple: Hypodense, solitary, linear laceration
Stellate: Hypodense, branching, linear lacerations
• Parenchymal and subcapsular hematomas (lentiform configuration)
Unclotted blood (35-45 HU) soon after injury
– NECT: May be hyperdense to normal liver
– CECT: Hypodense to enhancing normal liver tissue
Clotted blood (60-90 HU)
– Hyperdense to unclotted blood and normal liver
– May be hyperdense to unenhanced liver
– “Sentinel clot” helps to localize source of bleeding
• Active hemorrhage or pseudoaneurysm
CECT: Active hemorrhage
– Isodense to enhanced vessels
– Extravasated contrast materia l (85-350 HU) surrounding low-attenuation clot
• Hemoperitoneum: Perihepatic and peritoneal recess blood collections
Injury to bare area of liver may result in retroperitoneal, not intraperitoneal, bleeding
• Periportal tracking: Linear, focal, or diffuse periportal zones of decreased HU
Due to dissecting blood, bile, or dilated periportal lymphatics
Differential diagnosis: Overhydration; check for distended inferior vena cava (IVC)
– Increased venous pressure and transudation
• Areas of infarction
Small or large areas of low attenuation
Usually wedge-shaped; segmental or lobar
Intrahepatic/subcapsular gas (due to hepatic necrosis)
May be due to trauma itself or iatrogenic (following surgery or coil embolization for active bleeding)



 .
.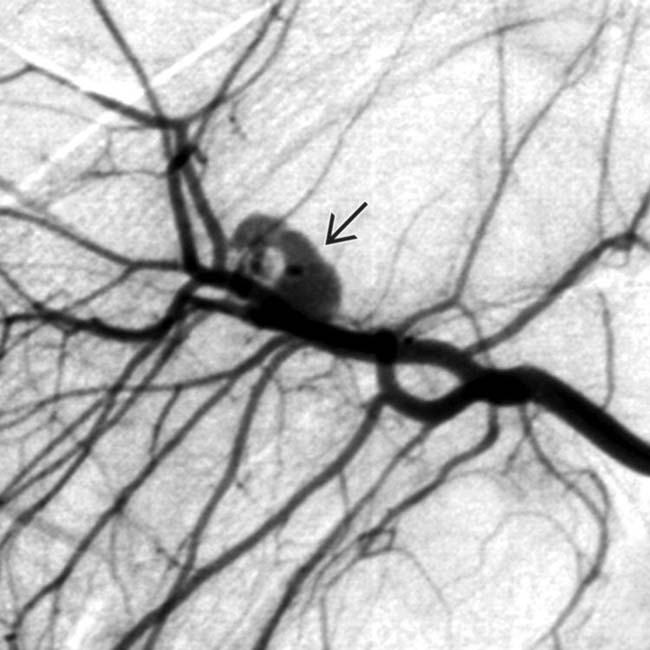
 , which was successfully treated with a coil embolization. The patient made an uneventful recovery without the need for a blood transfusion.
, which was successfully treated with a coil embolization. The patient made an uneventful recovery without the need for a blood transfusion.
 .
.
 into the peritoneal cavity along the hepatic capsule. Due to the acute intraperitoneal bleeding, urgent surgery was performed, which revealed an actively bleeding capsular artery.
into the peritoneal cavity along the hepatic capsule. Due to the acute intraperitoneal bleeding, urgent surgery was performed, which revealed an actively bleeding capsular artery.

























