Sliding (axial) hiatal hernia (HH): Gastroesophageal (GE) junction and gastric cardia pass through esophageal hiatus
Paraesophageal (rolling) hernia: Gastric fundus ± other parts of stomach herniate into chest
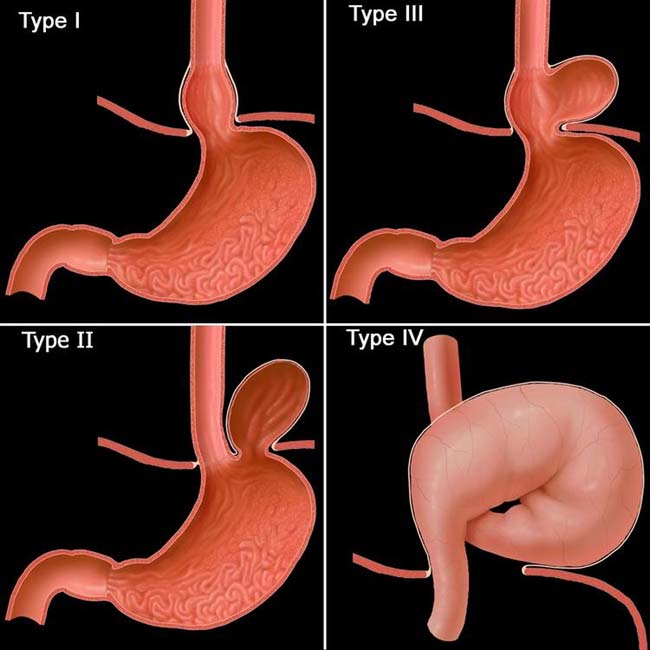
• Surgical classification
Type I: Sliding HH (only cardia in chest); most common type
Type II Paraesophageal (PEH): GE junction in normal position under diaphragm, fundus in chest (very rare)
Type III PEH: GE junction in chest, along with fundus ± other portions of stomach (2nd most common HH)
Type IV PEH: Intrathoracic stomach ± volvulus
• Type I (sliding HH): Signs on upper GI series
Lower esophageal mucosal (B) ring observed ≥ 2 cm above diaphragmatic hiatus
Often reducible in erect position
Numerous (> 6) longitudinal gastric folds within HH continue through hiatus into abdominal part of stomach
Gastric folds converging superiorly toward a point several centimeters above diaphragm
TOP DIFFERENTIAL DIAGNOSES
• Phrenic ampulla
• Postoperative change
• Pulsion diverticulum
CLINICAL ISSUES
• Medical treatment and lifestyle modification (treatment same as for gastroesophageal reflux disease [GERD])
• Increasing use of laparoscopic fundoplication to treat GERD and to repair all types of HH
(Left) Graphic outlines the surgical classification of hiatal hernias (HH). Type I is a sliding HH, and types II-IV are paraesophageal hernias. Type III is the 2nd most common type, but it is rare compared to type I (sliding HH).
(Right) Esophagram in a patient with type I sliding HH shows the lower esophageal sphincter, or phrenic ampulla, marked by the A ring proximally and the B ring distally. Just below the B ring is the herniated portion of the gastric cardia .
(Left) Film from a barium esophagram in a patient with type I sliding HH shows the gastroesophageal (GE) junction, marked by the B ring . Gastric folds extend up through the hiatus.
(Right) Esophagram in the same patient (supine position) reveals reflux . While reflux is commonly seen in patients with sliding HHs, it is uncertain whether the HH causes the reflux or vice versa.
TERMINOLOGY
Abbreviations
• Hiatal hernia (HH)
Definitions
• Protrusion of part of stomach through esophageal hiatus of diaphragm
IMAGING
General Features
• Best diagnostic clue
Fluoroscopy after barium meal showing some portion of stomach in thorax
• 2 general types
Sliding (axial)
– Gastroesophageal (GE) junction and gastric cardia pass through esophageal hiatus of diaphragm into thorax
Paraesophageal (rolling) hernia
– Gastric fundus ± other parts of stomach herniate into chest
• Surgical classification
Type I: Sliding HH (only cardia in chest)
Type II paraesophageal (PEH): GE junction in normal position (under diaphragm)

 Type II Paraesophageal (PEH): GE junction in normal position under diaphragm, fundus in chest (very rare)
Type II Paraesophageal (PEH): GE junction in normal position under diaphragm, fundus in chest (very rare) Type III PEH: GE junction in chest, along with fundus ± other portions of stomach (2nd most common HH)
Type III PEH: GE junction in chest, along with fundus ± other portions of stomach (2nd most common HH)

 Numerous (> 6) longitudinal gastric folds within HH continue through hiatus into abdominal part of stomach
Numerous (> 6) longitudinal gastric folds within HH continue through hiatus into abdominal part of stomach


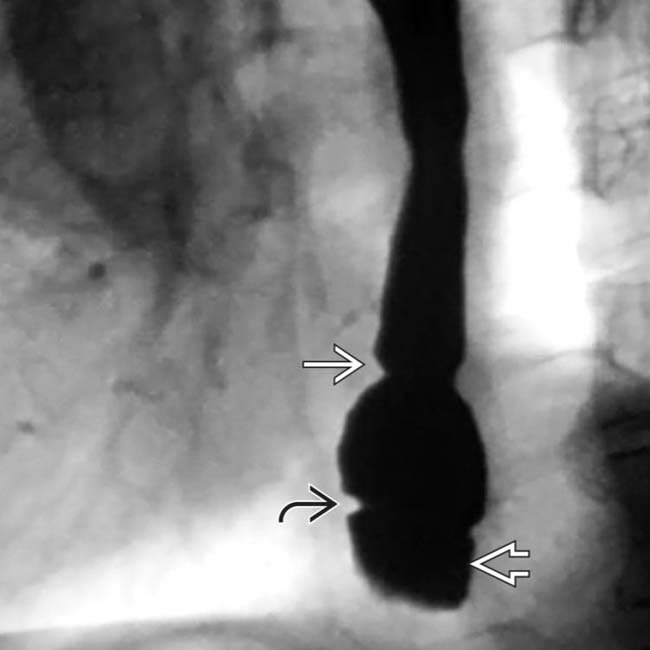
 proximally and the B ring
proximally and the B ring  distally. Just below the B ring is the herniated portion of the gastric cardia
distally. Just below the B ring is the herniated portion of the gastric cardia  .
.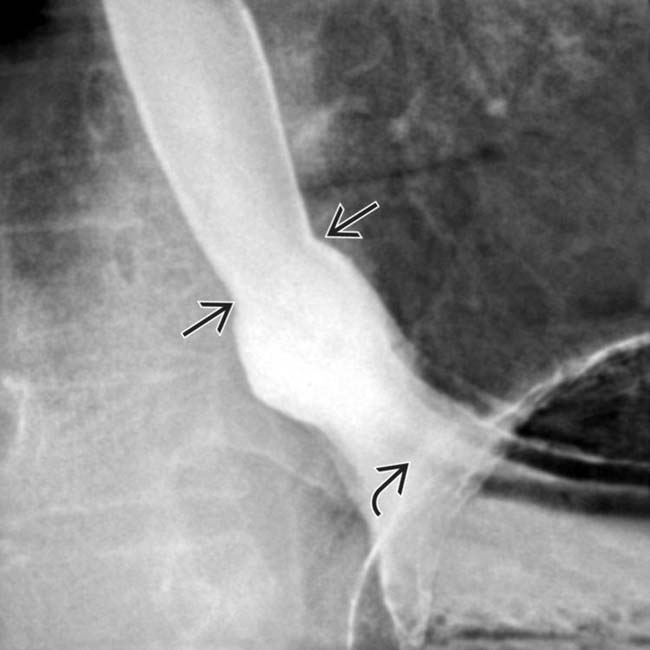
 . Gastric folds
. Gastric folds  extend up through the hiatus.
extend up through the hiatus.
 . While reflux is commonly seen in patients with sliding HHs, it is uncertain whether the HH causes the reflux or vice versa.
. While reflux is commonly seen in patients with sliding HHs, it is uncertain whether the HH causes the reflux or vice versa.




















