Hips and Proximal Femora
John H. Harris Jr.
GENERAL CONSIDERATIONS
The hip is a ball and socket joint consisting of the acetabulum and the head of the femur. The articulating (lunate) surface of the acetabulum is incomplete medially (acetabular notch) and is thickest superiorly to accommodate the pressure of the body weight when erect. This radiographically dense segment portion of the lunate surface must not be misinterpreted as the reactive sclerosis of degenerative joint disease.
The femoral head, which occupies the acetabular fossa, has a shallow concavity (fovea centralis) on its superomedial surface to which the ligamentum teres is attached. The ligamentum teres carries a small artery, the artery of the ligamentum teres, which supplies only approximately 10% of the blood supply to the femoral head. This has an important relationship to subcapital femoral neck fractures that is discussed and illustrated in the body of this chapter.
The femoral neck including the intertrochanteric crest and the proximal femoral shaft are, anatomically, not considered part of the hip. However, because fractures of these segments of the proximal femur are clinically referred to as “hip fractures,” they are included in this chapter.
It is necessary to realize that the “frog leg lateral” of the hip is not the true lateral projection of the proximal femur but is simply an externally rotated view. The “groin” or cross- lateral projection of the proximal femur is the only true lateral orthogonal view of the hip. This important fact is illustrated in the body of this chapter.
The capital femoral epiphysis appears during the first year of life, the apophysis of the greater trochanter appears before the fifth year, and that of the lesser trochanter during the 13th year. All of these centers unite with the femur during the 18th to 20th years.
A homily aptly describes the relationship of the femoral head to the femoral neck. The femoral head rests symmetrically on the femoral neck like a scoop of ice cream squarely placed in an ice cream cone. In both the anteroposterior (AP) and lateral radiographs, the sweep of the cortex extending from the neck to the head is smooth and symmetrical (Fig. 19.1). Before the fusion of the head with the neck, the capital femoral epiphysis sits squarely on the metaphysis of the femoral neck. Asymmetry of the head with respect to the neck, even if seen in only one projection, is an abnormal finding and represents either slipped capital femoral epiphysis (SCFE) in an adolescent or a subcapital fracture in an adult.
The routine examination of the hip includes AP (Fig. 19.1A), lateral (Fig. 19.1B), and externally rotated (Fig. 19.1C) projections. The AP view of the hip must include a clear depiction of the greater trochanter (Fig. 19.1D). Distinction must be made between true lateral and frog leg lateral projections of the hip. The true (horizontal beam, cross-table, groin) lateral projection is obtained with the patient supine and the injured lower extremity in full extension. The opposite, uninvolved hip and knee are flexed approximately 90 degrees each, and the ipsilateral foot is supported off the radiographic table
by a low stool or box. The x-ray tube is then positioned so that the beam is parallel to the table top, with the central ray directed mediolaterally parallel to and in the same vertical plane as the inguinal crease. The cassette is firmly positioned against the flank between the iliac crest and the 12th rib on the injured side perpendicular to the central ray. This beam cassette geometry results in the true lateral radiograph of the hip (Fig. 19.1B), which is essential for the complete evaluation of injuries of the proximal portion of the femur.
by a low stool or box. The x-ray tube is then positioned so that the beam is parallel to the table top, with the central ray directed mediolaterally parallel to and in the same vertical plane as the inguinal crease. The cassette is firmly positioned against the flank between the iliac crest and the 12th rib on the injured side perpendicular to the central ray. This beam cassette geometry results in the true lateral radiograph of the hip (Fig. 19.1B), which is essential for the complete evaluation of injuries of the proximal portion of the femur.
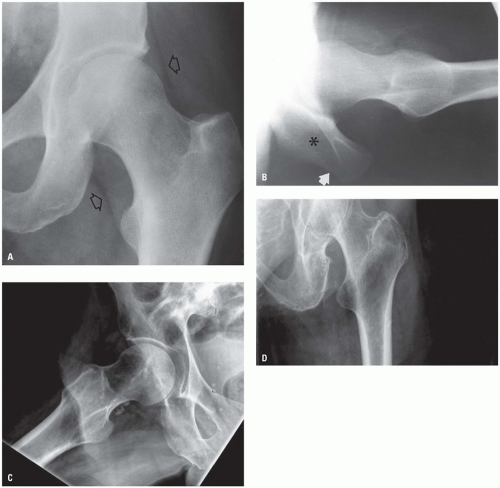 Figure 19.1. AP and lateral radiographs of the hip. A: On the frontal projection, linear lucencies (open arrows) representing fascial planes covering the gluteus minimus (superior open arrow) and the iliopsoas (inferior open arrow) muscles are frequently mistakenly thought to outline the hip joint capsule. The capsule is deep to each of these muscles. B: On the groin lateral projection, the angle subtended by the intersection of the long axis of the femoral neck and the proximal femoral shaft should be approximately 120 degrees, with the apex posteriorly directed. The horizontal beam lateral projection can always be oriented properly using the ischium (asterisk) and its tuberosity (white arrow) as landmarks. C: Frog leg projection: The frog leg projection results in an approximately 45-degree oblique view of the proximal femur. It is not a lateral view as suggested by the misnomer “frog leg lateral.” D: The frontal view of the proximal femur must include a true depiction of the greater trochanter. |
The “frog leg lateral” projection, on the other hand, is actually an oblique projection of the proximal portion of the femur and is obtained with the patient supine and the femur abducted and externally rotated. The x-ray tube is vertically positioned with respect to the patient (and the radiographic table) and centered over the hip joint. The resultant radiograph depicts the femur in midposition between true AP and true lateral positions. The frog leg radiograph is inappropriate in the evaluation of the patient with an acute injury of the hip because of the manipulation of the hip necessary to achieve this view and because neither the femoral neck-shaft angle nor the greater trochanter can be adequately evaluated.
In the frontal projection of the hip (Fig. 19.2), the lateral weight-bearing portion of the acetabular roof is thicker and more densely sclerotic than the other radiographically visible portions of the acetabular concavity. The transition from the weight-bearing portion of the roof to the adjacent surface of the fossa is normally abrupt and represents the free margin of the lunate surface. The posterior acetabular rim, which is usually visible through the density of the femoral head, appears as a thin, faint, occasionally slightly undulating linear density that extends inferomedially from the lateral free margin of the acetabular roof. The anterior acetabular rim, which is less often visible, is medial to the posterior rim and has a similar oblique orientation. The inferior portion of the acetabular fossa, with the exception of the teardrop shadow, is not visible radiographically because of the acetabular notch.
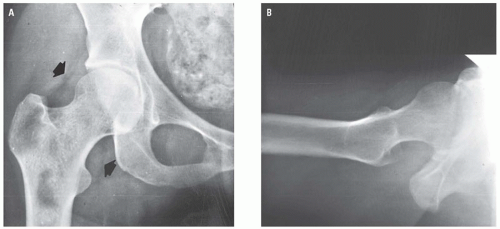 Figure 19.2. Normal adult hip in AP (A) and horizontal beam groin lateral (B) projections. On the AP radiograph (A), the superolateral arrow indicates the fascial plane covering the gluteus minimus muscle; the inferomedial arrow, the iliopsoas muscle. |
The femoral head arises from a single ossification center that appears at the end of the first year of life (Fig. 19.3) and fuses with the femoral neck at approximately age 18 years. The fused physeal scar identifies the anatomic neck of the femur.
In the straight frontal, externally rotated oblique, and groin lateral projections, the femoral head is normally symmetrically situated on the femoral neck. The convexity of the subchondral cortex of the head is normally congruent with the concavity of the lunate surface of the acetabulum. The fovea centralis (Fig. 19.2) is a short concavity located in
the convexity of the femoral head into which inserts the ligamentum teres (ligament of the head of the femur). This ligament generally contains a small artery that provides approximately 10% of the blood supply of the femoral head.
the convexity of the femoral head into which inserts the ligamentum teres (ligament of the head of the femur). This ligament generally contains a small artery that provides approximately 10% of the blood supply of the femoral head.
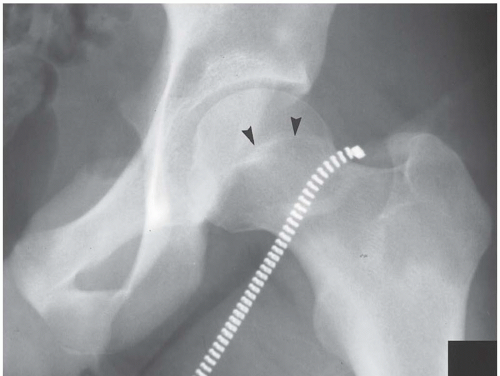 Figure 19.3. AP projection of an adolescent hip. The thin curvilinear density (arrowheads) is the “scar” of the fused proximal femoral physis. |
HIP TRAUMA
Hip Dislocation
The most common mechanism of injury in dislocation of the hip is abrupt deceleration such as occurs in a motor vehicle accident in which the knee strikes the dashboard with the force of impact transmitted along the femoral shaft to the femoral head. If, at the moment of impact, the thigh is adducted, the femoral head may be dislocated posterolaterally, without (Fig. 19.4) or with (Fig. 19.5) fracture of the posterior acetabular lip. Because the mechanism of injury of posterior dislocation of the hip also usually includes an element of superior displacement, the femoral head will come to rest in some degree of superior displacement with respect to the acetabular fossa. Its posterior location is established on the horizontal beam lateral projection (Fig. 19.4). Anterior dislocation of the hip represents 10% to 15% of traumatic hip dislocations.1, 2, 3, 4 In anterior dislocation, the femur may be displaced anteriorly and medially toward the superior pubic ramus (Fig. 19.6) or toward the obturator foramen (Fig. 19.7).5 In this instance, an impaction of the femoral head on the dense, blunt anteroinferior arc of the anterior acetabular rim may produce a Hill-Sachs type of fracture of the femoral head (Fig. 19.7B). Medial displacement of the femoral head with respect to the acetabulum, in the frontal projection (Fig. 19.6A), is characteristic of anterior dislocation and distinguishes it from the typical superolateral position of the posteriorly dislocated hip. The anterior dislocation will be confirmed in the horizontal beam lateral radiograph (Fig. 19.6B).
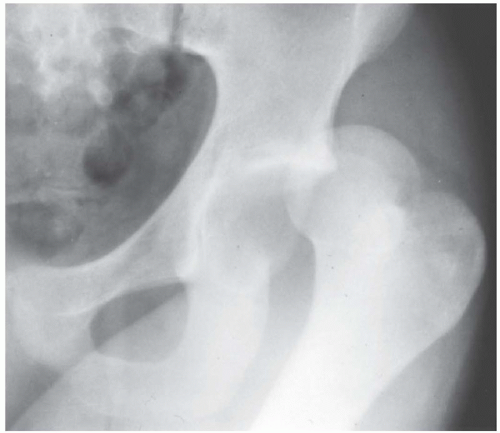 Figure 19.4. Posterior dislocation of the left hip without associated fracture. |
The configuration of the posterior rim of the acetabulum resembles the blade of a hatchet or axe. Consequently, as described and illustrated, the thin edge of the rim is subject to fracture (Figs. 19.5 and 19.8) with posterior hip dislocation. When, because of the direction of the dislocating force, the posterior acetabular rim functions as a cutting edge, the impacting force is dissipated on the femoral head, resulting in capital femoral epiphyseal separation in adolescents (Fig. 19.9) or fracture of the femoral head in adults (Figs. 19.10 and 19.11). The cardinal signs of femoral head fracture on the initial examination include a flat segment of the femoral head without its normal subchondral cortex and separate fracture fragment(s) within the acetabular fossa (Figs. 19.10 and 19.11). The role of computed tomography (CT) and 3-D CT in evaluation of injuries of the hip is illustrated in a patient with
bilateral posterior dislocations of the hip and bilateral femoral head fractures (Fig. 19.12) in which the 3-D CT images provide unambiguous spatial orientation and relationships of the intra-articular fragments and the dislocated femora with respect to the acetabular fossae.
bilateral posterior dislocations of the hip and bilateral femoral head fractures (Fig. 19.12) in which the 3-D CT images provide unambiguous spatial orientation and relationships of the intra-articular fragments and the dislocated femora with respect to the acetabular fossae.
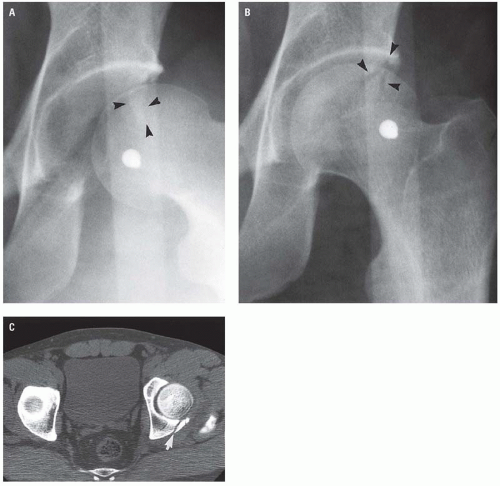 Figure 19.5. Posterior fracture dislocation. A: On the AP radiograph, the dislocation of the femoral head should be obvious because of the gross incongruity of its cortical margins with that of the acetabulum. A faint, vertical density (arrowheads) represents a minimally displaced posterior rim fragment. B: The fracture line (arrowheads) is more evident on the postreduction radiograph. C: The posterior rim fracture (arrow) is confirmed on CT. |
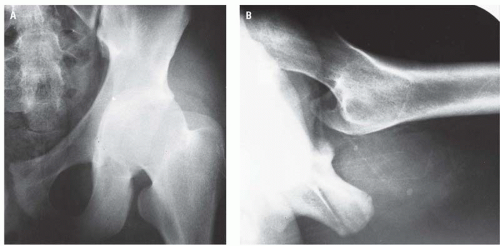 Figure 19.6. Anterior dislocation of the hip in which the femoral head is displaced medially and toward the superior pubic ramus (A). The anterior dislocation is confirmed in the horizontal beam lateral projection (B). |
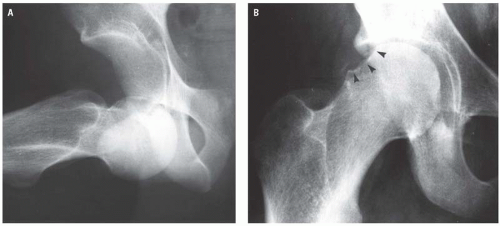 Figure 19.7. “Obturator” variety of anterior hip dislocation with associated compression fracture of the femoral head. A: In the frontal projection, the femoral head is anteriorly dislocated and directed toward the obturator foramen. With the femoral head in this position relative to the acetabulum, it is entirely reasonable to suspect the possibility of a femoral head compression fracture. B: In the postreduction radiograph, the femoral head compression fracture (arrowheads) is clearly evident. |
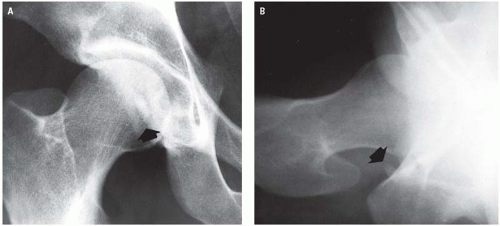 Figure 19.8. Isolated fracture of the posterior acetabular lip. Arrows indicate the posterior lip fragment in both frontal (A) and horizontal beam lateral (B) projections. There is no evidence of associated dislocation. |
Proximal Femoral Fractures
Fractures of the proximal end of the femur may be classified based on their relationship to the hip joint capsule—that is, intracapsular (subcapital, transcervical, and basicervical) or extracapsular
(intertrochanteric, subtrochanteric, and trochanteric)6 —or based on the geographic location of the fracture, that is, femoral neck (subcapital, transcervical, and basicervical), intertrochanteric (subclassified based on number of fragments), trochanteric, and subtrochanteric.7, 8, 9 Intracapsular fractures have a significantly higher incidence (10% to 35%)6, 9, 10 of aseptic (avascular) necrosis of the femoral head than extracapsular fractures. Posttraumatic avascular necrosis of the femoral head is greatest in fractures in which there is displacement of the fragments. Extracapsular fractures, on the other hand, usually heal well but are more likely to be unstable, particularly the three- and four-part intertrochanteric fractures.
(intertrochanteric, subtrochanteric, and trochanteric)6 —or based on the geographic location of the fracture, that is, femoral neck (subcapital, transcervical, and basicervical), intertrochanteric (subclassified based on number of fragments), trochanteric, and subtrochanteric.7, 8, 9 Intracapsular fractures have a significantly higher incidence (10% to 35%)6, 9, 10 of aseptic (avascular) necrosis of the femoral head than extracapsular fractures. Posttraumatic avascular necrosis of the femoral head is greatest in fractures in which there is displacement of the fragments. Extracapsular fractures, on the other hand, usually heal well but are more likely to be unstable, particularly the three- and four-part intertrochanteric fractures.
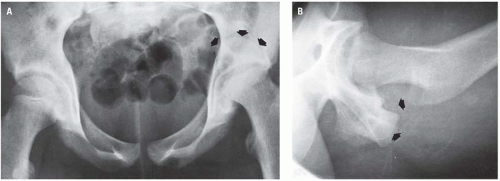 Figure 19.9. Capital femoral epiphyseal separation-posterior dislocation. A: In the frontal projection, the capital femoral epiphysis is indicated by the arrows. The femoral neck has remained within the acetabulum, and its metaphyseal plate relates to the acetabular fossa. B: In the horizontal beam lateral radiograph, the arrows indicate the posteriorly dislocated capital femoral epiphysis. |
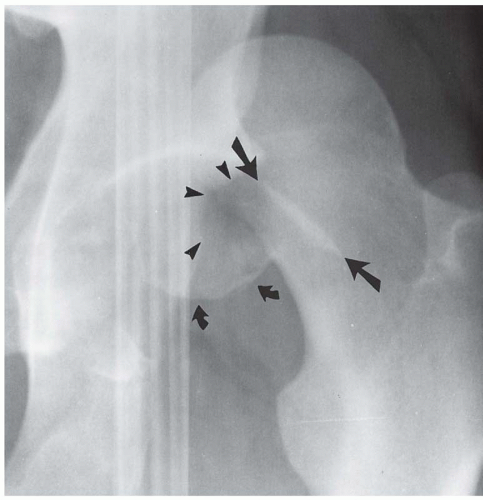 Figure 19.10. Concomitant posterior column (rim) and femoral head (curved arrows) fractures associated with posterior dislocation of the hip. Straight arrows indicate the rim fragment, and arrowheads indicate its defect in the posterior acetabular rim. |
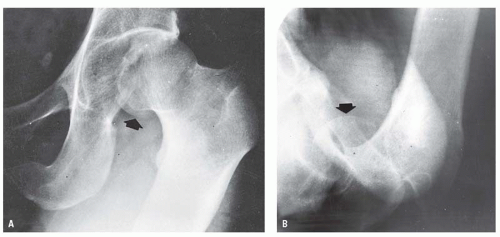 Figure 19.11. Posterior dislocation of the left hip with a large femoral head fragment. In the frontal projection (A), the dislocation is obvious. The faint crescentic density (arrow) inferior to the femoral head is a separate femoral head fragment confirmed to be within the acetabulum in the horizontal beam lateral radiograph (B). |
The hip joint capsule extends anteriorly from the anteroinferior iliac spine and the iliopectineal eminence of the innominate bone to the intertrochanteric line of the femur. The hip capsule is attached posteriorly to the acetabulum approximately 5 to 6 mm above its rim, distally to the femoral neck well above the intertrochanteric crest, and inferomedially to the femoral neck above the lesser trochanter (Fig. 19.13). The trochanters are extracapsular.
The normal radiographic skeletal and soft tissue anatomy of the hip is repeated (Figs. 19.1 and 19.14) here for ease of comparison. Contrary to an often repeated imprecision, the soft tissue linear lucencies, superolateral and inferomedial to the femoral head and neck (Fig. 19.1A), do not indicate the hip joint capsule. Rather, they represent areolar tissue in the fascial plane covering the gluteus minimus muscle superiorly and the tendon of the iliopsoas muscle inferiorly. A large intrasynovial fluid collection may displace the lucent stripes or make them convex. However, it must be clearly understood that normal fascial planes about the hip joint do not exclude intrasynovial pathology. This is particularly true in the instance of young children who refuse to bear weight on one leg and in whom septic arthritis (pyarthrosis) is clinically suspected. This circumstance requires scintigraphy CT or Magnetic resonance imaging (MRI) for further evaluation. This recommendation must be transmitted to the referring physician.
Intracapsular proximal femoral fractures include the subcapital, transcervical, and basicervical. Subcapital fractures are commonly extremely subtle and, in AP projection, may be manifested only by superimposition of the rim of the base of the femoral head upon the femoral neck (Fig. 19.15). Typically in subcapital fractures, the femoral head rotates clockwise on the right and counterclockwise on the left within the acetabulum. The rotational displacement of the head results in impaction at the medial end of the fracture line and flattened normal neck-head relationship laterally (Fig. 19.16A-D), whereas the inferior neck-head anatomy appears normal with intact cortex (Fig. 19.17A). In the horizontal beam lateral projection, displacement of the femoral head, which is usually posterior with respect to the neck, in association with disruption of the anterior cortex (Fig. 19.17B) confirms the diagnosis. Impaction of the femoral head on the neck will produce an indistinct broad band of relative increased density in the subcapital region
(Fig. 19.18




(Fig. 19.18
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
