Fig. 29.1
IRGUS system display. The pancreas (yellow) and kidney (orange) are shown in the ultrasound plane (top left) and the reformatted preoperative CT (top right). Bottom. 3D view of the patient anatomy with the EUS probe shown in blue and black and the ultrasound plane shown in green, close to the pancreatic tumor
The IRGUS system is efficient and accurate at identification of probe position and image interpretation. This allows for the endoscopist to quickly visualize anatomic structures without losing echoendoscope image orientation (especially when the sonographic image is degraded by calcifications, artifacts, or poor surface contact). Thus, IRGUS appears to have the capability to shorten procedure times, minimizing sedation requirements and overall procedure times. Use of the IRGUS system is also expected to lead to improvement in lesion targeting for echoendoscopic biopsy or fine-needle aspiration with the potential to enhance tissue sampling for better diagnosis of disease.
A goal of these early tests in humans has been to quantify the anatomic differences in the pancreas for this population of patients with diagnosed cancer of the organ. Figure 29.2 shows CT-derived models of the pancreas for four patients. It is observed that, despite the presence of disease, the pancreas has a similar shape and size, which improves the likelihood that standardized models of the diseased pancreas may be constructed, which, in turn, will permit the implementation of systematic warping of the CT data to accommodate changes induced by gravity when the patient is in the left lateral decubitus position.
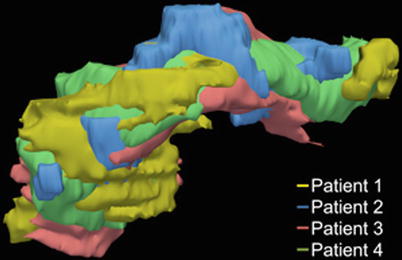
Fig. 29.2
Surface models of the pancreas segmented from the CT examinations of four patients after alignment in the same coordinate frame. Each color represents a different patient. The shape and size of the pancreas are similar among these patients
These are the current limitations of the current IRGUS system:
The accuracy of probe placement was generally limited to the range of 0.5–1.0 cm, depending on the patient anatomy, patient position (supine or left lateral decubitus), and other factors. This is larger than might be clinically useful and is likely due to errors in probe/patient registration to the CT model.
The standard practice of performing pancreas FNA requires the patient to be in the left lateral decubitus position. The CT scan of the patient is obtained in the supine position. Due to the patient lying on his/her side, the organs can shift within the retroperitoneal space due to the gravitational force and viscoelastic nature of organs, as shown in Fig. 29.3.
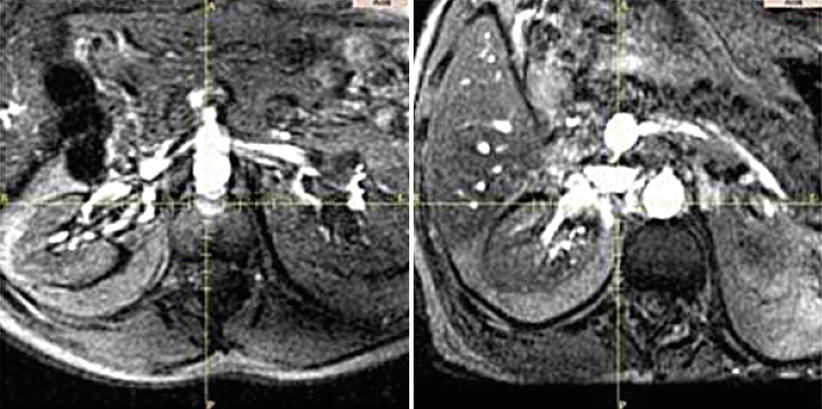
Fig. 29.3
MRI scans of a volunteer patient showing the organ deformation. Left – supine; right – decubitus
The software architecture (implemented in 3D Slicer version 2.6 (see Chap. 19)) is not designed to support “real-time” registration correction nor is it adequately versatile to support trackers and interfaces from various vendors. Preliminary work includes port of key IRGUS components to a newer 3D Slicer architecture. In particular, we have implemented the OpenIGTLink [31] networking protocol to pass real-time ultrasound image and 3D tracker data into the 3D Slicer software for display. In general these challenges will be overcome by better architecture and task partitioning in the next few years and then likely be resolved by the continual increase in processing speeds.
Image-Registered Endoscopic Ultrasound-guided fine-needle aspiration also appears to be an easily implemented approach for characterizing suspicious lesions in other sections of the torso. Fernandez-Esparrach et al. [32] showed that the same system used for IRGUS has similar performance advantages in locating selected anatomic targets in the mediastinum.
Image-Registered Ureteroscopy
Calculi (stones) in the urinary tract are common in the US population; they occur in nearly one million patients every year. The technique used to treat stones depends on the size and location. Ureteroscopy is often used in the treatment of stones by first passing a cystoscope through the urethra into the bladder. The ureter and collecting system are then cannulated using wires under fluoroscopic guidance. The ureteroscope is then advanced over the wire to the upper collecting system. Once the urologist locates the stone, either in the ureter or kidney, it can be fragmented using a holmium:YAG laser, which acts through an optic fiber introduced through the ureteroscope.
Alternatively, a percutaneous approach may be adopted for large renal stones or in patients with anatomic aberrancies to provide direct access to the stones. In this case, the collecting system is accessed through a percutaneous puncture. A guide wire is inserted through the percutaneous puncture location into the calices. The tract is dilated and either a rigid or flexible (cystoscope and ureteroscope) nephroscope is inserted into the collecting system. Once the stone is located, either a pneumatic ultrasound lithotripter or the holmium:YAG laser is passed through the lumen of the scope to fragment the stones. This method requires puncturing of the kidney using a needle percutaneously, which could in turn result in puncturing neighboring vascular structures or inadvertent entering of the system in a position that can result in damage to the kidney.
For patients with a solitary kidney or a transplant kidney, the challenges amplify due to the requirement of preserving kidney function. The challenges of navigating equipment into a displaced ureteral orifice or throughout a renal pelvis to access the stones have motivated the development of an Image Registration (or “GPS”) navigation system to visualize the cystoscope within the bladder and guide it to the displaced ureteral orifices and also to guide a ureteroscope either antegrade or retrograde throughout the calices of the kidney (see Fig. 29.4) to treat multiple stones or stones in multiple calyces. The navigation system also enables visualization and pre-procedure planning to assess the difficulty of gaining access through the transurethral approach or accessing the stone percutaneously (Fig. 29.5).
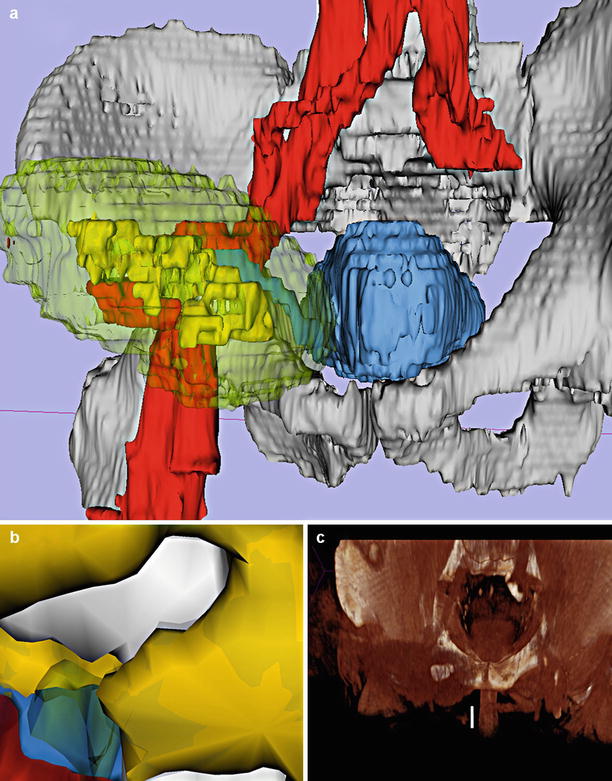
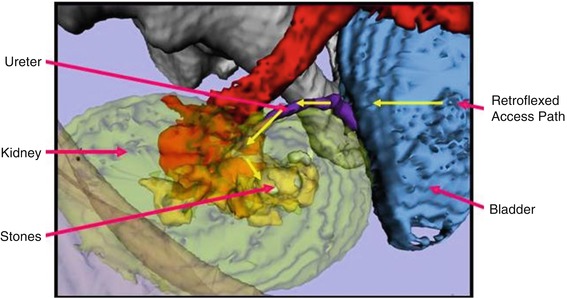
Fig. 29.4
(a) Global anatomic view showing a transplanted kidney, calices, stone, bladder, aorta, ureter, and skeleton. (b) Virtual endoscopic view showing a local magnified view of the stone, calices, ureter, and blood vessels. (c) Volume rendered view from a wingman’s perspective (Courtesy J. Jayender)
Fig. 29.5
Plan of ureteroscope access to the stones in a transplanted kidney, showing necessary retroflexed approach. (Courtesy J. Jayender)
Image Registration for Natural Orifice Transluminal Endoscopic Surgery (NOTES)
In creating viable NOTES procedures, the navigation of instruments safely and effectively in the body was appreciated and recognized as a key requirement [33]. The technique of real-time Image Registration may help address this need. Here are examples of recent animal and cadaver model studies:
Fernandez-Esparrach et al. compared two sites for transgastric access and one for transcolonic access to the peritoneum using a porcine model and CT-based image-registered navigation system to identify preselected targets [34]. The operator display for Image-Registered NOTES (IR-NOTES) included a 3D model and a simulated (virtual) endoscopic view as shown in Fig. 29.6. The results were consistent (but not with statistical significance) with the hypothesis that IR-NOTES procedures had fewer complications but did demonstrate that the operator moved the instruments more smoothly when IR-NOTES guidance was provided.
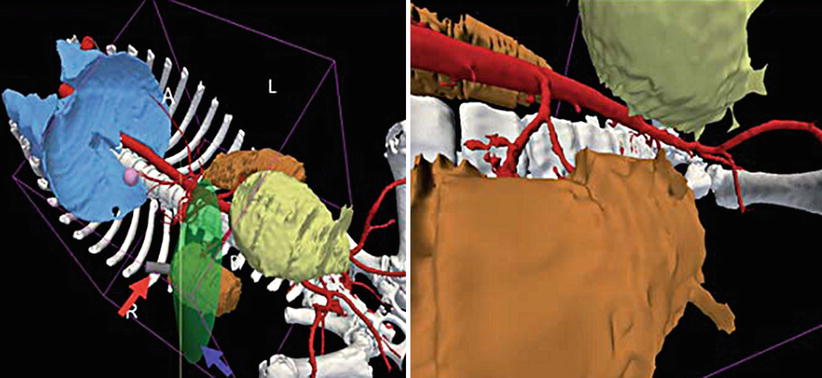
Fig. 29.6
Left, image-registered display of the endoscope field of view (translucent green cone), and right, virtual endoscopic view constructed from the 3D model, looking along the side of the right kidney toward the pelvis (Courtesy: Raúl San José Estépar)
Azagury et al. endoscopically targeted 15 intra-abdominal organs with and without IR-NOTES via both transgastric and transcolonic routes, by three endoscopists with different levels of expertise, in three human cadavers [35]. Without IR-NOTES, 11.7 % of the targets were not reached, compared to 1 % in the IR-NOTES evaluation (P = 0.002). The IR-NOTES system enhanced both navigation efficacy and ease of intra-abdominal NOTES exploration for operators of all levels.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


