 with diffuse wall thickening
with diffuse wall thickening  , multiple gallstones
, multiple gallstones  , and pericholecystic fluid
, and pericholecystic fluid  . Sonographic Murphy sign was positive. These are classic clinical and US features of acute cholecystitis.
. Sonographic Murphy sign was positive. These are classic clinical and US features of acute cholecystitis.
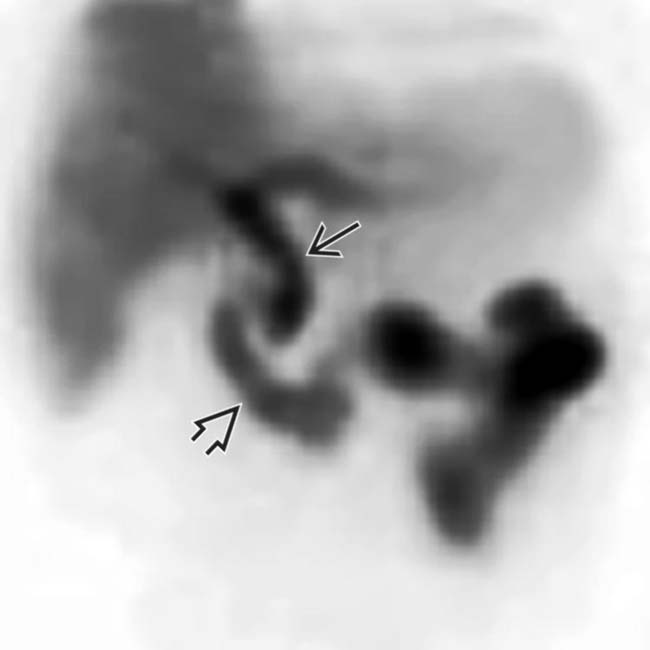
 and bowel
and bowel  but not into the gallbladder, indicating obstruction of the cystic duct and indirectly suggesting acute cholecystitis.
but not into the gallbladder, indicating obstruction of the cystic duct and indirectly suggesting acute cholecystitis.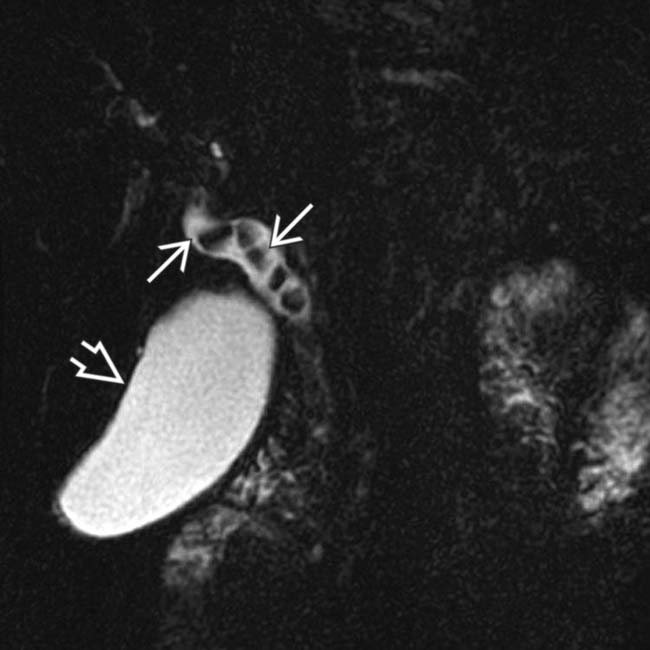
 within the dilated CBD. The gallbladder is marked
within the dilated CBD. The gallbladder is marked  for identification.
for identification.
 . During the same procedure, a papillotomy was performed with balloon sweep clearing of the ductal stones followed by placement of a temporary plastic biliary stent. All symptoms resolved.
. During the same procedure, a papillotomy was performed with balloon sweep clearing of the ductal stones followed by placement of a temporary plastic biliary stent. All symptoms resolved.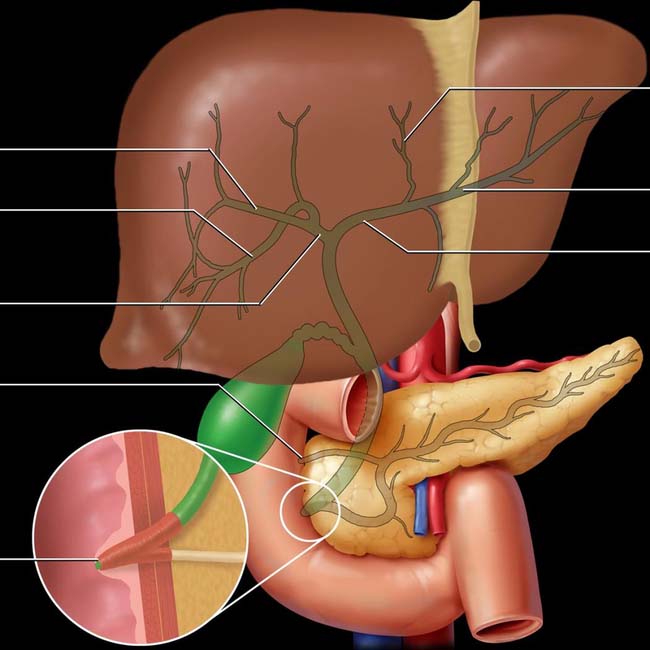
Right posterior-caudal (segments 6 and 7)
Right hepatic duct
Minor papilla
Major papilla (hepatoduodenal papilla)
Ducts to segment 4
Ducts to segments 2 and 3
Left hepatic duct
(Top) Note the distribution of the larger intrahepatic bile ducts. The CBD usually joins with the pancreatic duct in a common channel or ampulla (of Vater) but may enter the major duodenal papilla separately. The distal bile duct has a sphincteric coat of smooth muscle, the choledochal sphincter (of Boyden), which regulates bile emptying into the duodenum. When contracted, this sphincter causes bile to flow retrograde into the gallbladder for storage. The common hepaticopancreatic ampulla may be surrounded by a smooth muscle sphincter (of Oddi).
 and common duct
and common duct  due to the presence of a biliary stent (not shown). The GB wall is normal.
due to the presence of a biliary stent (not shown). The GB wall is normal.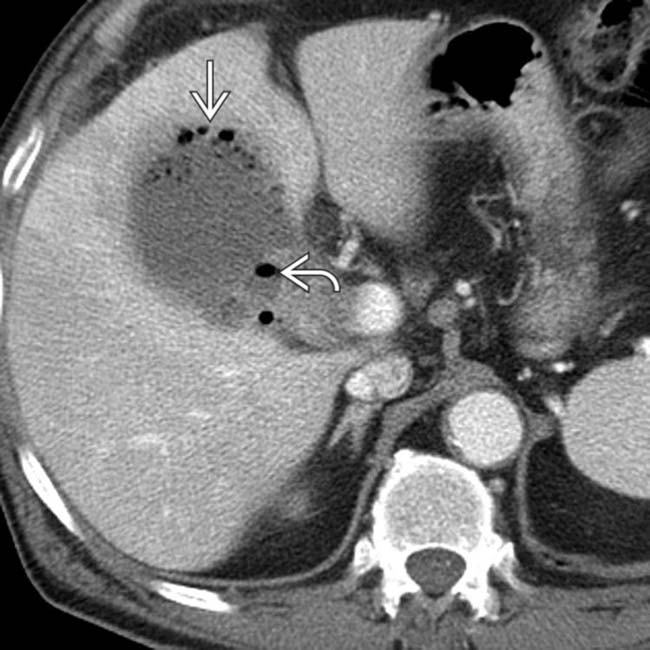
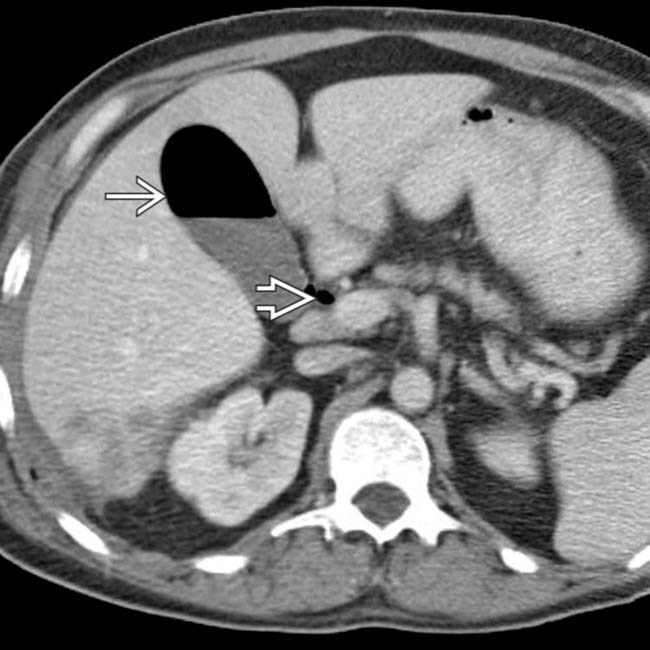
 and wall of the GB
and wall of the GB  with a hazy margin where the GB abuts the liver. This emphysematous cholecystitis was treated urgently with percutaneous cholecystostomy and later with cholecystectomy.
with a hazy margin where the GB abuts the liver. This emphysematous cholecystitis was treated urgently with percutaneous cholecystostomy and later with cholecystectomy.
 with an acoustic shadow
with an acoustic shadow  and a thickened GB wall (calipers). These findings, along with a positive sonographic Murphy sign, are diagnostic of acute cholecystitis.
and a thickened GB wall (calipers). These findings, along with a positive sonographic Murphy sign, are diagnostic of acute cholecystitis.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


