Bladder cancer requiring cystectomy
Neurogenic bladder that threatens renal function
Severe radiation injury to urinary bladder
Intractable incontinence in females
Chronic pelvic pain syndromes
Types of urinary diversions performed today include:
Noncontinent, cutaneous diversion (conduit)
Continent, cutaneous diversion (pouch)
Continent urinary diversion to native urethra (neobladder, orthotopic reconstruction)
Noncontinent Cutaneous Urinary Diversion
Ileal Conduit
Noncontinent cutaneous urinary diversion with a small bowel segment is a standard technique with less complications (Fig. 14.1a–c).
Fig. 14.1
Noncontinent ileal conduit diversion. (a) Schematic drawing illustrates ileal conduit urinary diversion. (b) Retrograde contrast injection through the stoma of the ileal conduit outlines the urinary reservoir. (c) Axial contrast-enhanced CT demonstrates ileal conduit urinary diversion. The conduit is in the right lower quadrant (arrow) and arrowhead points to stoma
Distal 15–20 cm of ileum is commonly used. Segment of bowel is anastomosed to anterior abdominal wall to form a stoma to which an ostomy bag can be attached for urine drainage and ureters are attached to the other end of the bowel segment.
Cutaneous Ureterostomy
This is rarely performed and more commonly performed in pediatric patients as a temporary step before definitive procedure (Fig. 14.2).

Fig. 14.2
Cutaneous ureterostomy. Plain film radiograph of a 72-year-old patient with history of colon cancer and nonfunctioning right kidney. Nephroureteral stent (arrow) is present within the left-side ureterostomy
Ureters are directly anastomosed to the body wall (cutaneous ureterostomy).
Continent Cutaneous Urinary Diversions
Most are accomplished using three reservoirs: ascending colon, ileum, or a combination of both continuous cutaneous reservoirs involving a continent abdominal wall stoma.
Requires antireflux mechanism by submucosal tunneling ureteral-tenial implants, an intussuscepted nipple valve, or an afferent isoperistaltic ileal loop.
Continent diversions include Indiana, Mainz, Kock, and UCLA (University of California at Los Angeles) pouch.
(a)
Indiana Pouch
Most commonly performed continent urinary diversion.
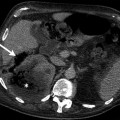
Ascending colon acts as a reservoir (Fig. 14.3a, b) and terminal ileum acts as efferent limb (Fig. 14.3c).
Fig. 14.3
Indiana pouch. (a) Schematic drawing illustrates Indiana pouch. Right colon acts as a reservoir, and ileum is used as an efferent limb to form the stoma. Ureters are implanted in the right colon that serves as reservoir. (b) Axial contrast-enhanced CT reveals right colon (arrow) serving as a reservoir. (c) Terminal ileum (arrow) acts as efferent limb. (d) Efferent limb externalized to form cutaneous stoma (arrow) in RLQ
Efferent limb externalized to form cutaneous stoma in RLQ (Fig. 14.3d). Surgically, a one-way valve is created to prevent the outflow of urine from the stoma. Patient does not have to wear a urinary bag but has to catheterize the stoma to empty the reservoir every 4–6 h.
The bowel segment used is detubularized. The purpose of detubularization is to create a reservoir with high capacity; shape is of secondary importance.
Efferent nipple not visualized on pouchography and CT in contrast to Mainz and UCLA pouch.
(b)
Mainz Pouch
This orthotopic bladder replacement technique uses cecum, ascending colon, and terminal ileum to construct reservoir (Fig. 14.4).
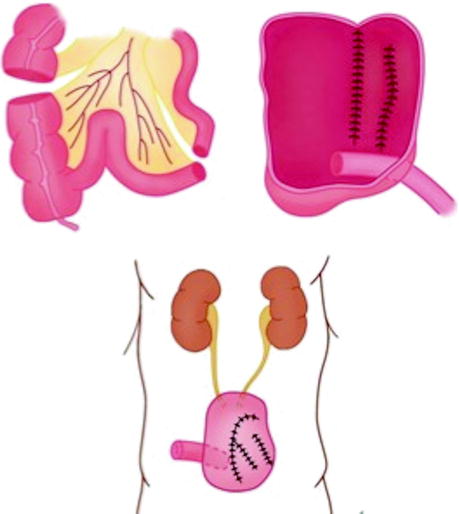
Fig. 14.4
Mainz pouch. Schematic drawing illustrates Mainz pouch. Pouch is constituted from right colon, cecum, and distal ileum
It has been further modified to Mainz II pouch surgery. Rectosigmoid plication creates Mainz II pouch.
Ureters are implanted in rectosigmoid reservoir with submucosal antirefluxing tunnel.
Urine outflow occurs during defecation.
(c)
Kock Pouch
Two 1-way nipple valves with associated afferent and efferent limbs (Fig. 14.5).
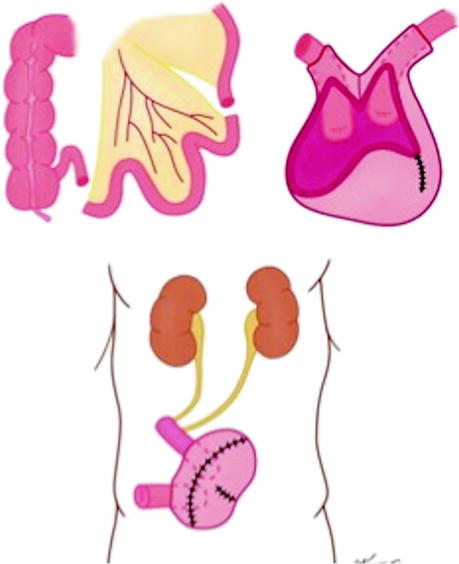
Fig. 14.5
Schematic drawing illustrates Kock pouch. Reservoir made of detubularized ileal loop for larger volume
Reservoir made of detubularized ileal loop for larger volumes.
Distal ureters implanted at afferent ureter.
Efferent limb as cutaneous stoma.
Most reconstructive surgeons have abandoned the continent Kock ileal reservoir largely because of the significant complication rate associated with the intussuscepted nipple valve.
(d)
University of California Los Angeles (UCLA) Pouch
Right colon is used as pouch with intussusception of terminal ileum and ileocecal valve that maintains continence mechanism (Fig. 14.6).
Fig. 14.6
Schematic drawing illustrates UCLA pouch. Urinary conduit is formed from right colon with intussusception of terminal ileum and ileocecal valve
Distal ileum serves as efferent limb.
Imaging findings of UCLA pouch are similar to Mainz pouch.
(e)
Miami Pouch
The reservoir is made from a small portion of terminal ileum, the ascending colon, and the proximal transverse colon.
In this technique, continence is maintained by reinforcing the ileocecal segment with three circumferential silk sutures.
This procedure provides reduced pouch pressure, less reflux, and reduced incontinence.
(f)
Studer Pouch
Studer pouch was introduced in 1989.
Reservoir has spherical shape with low pressure and constituted from four cross-folded ileal detubularized segments.
Ureters are directly anastomosed to isoperistaltic ileal segment forming an antireflux mechanism.
(g)
Charleston Pouch
Charleston pouch is a continent urinary diversion technique.
In this urinary diversion, reservoir is constructed from a detubularized colon and distal ileum.
Appendix is used as efferent limb to create the stoma at the umbilicus (Fig. 14.7a–c).
Fig. 14.7
Charleston pouch. (a) Gray-scale ultrasound demonstrates Charleston pouch. (b) Loopogram reveals filling of the reservoir constituted from distal ileum and right colon. (c) Axial computed tomography demonstrates Charleston pouch with appendix (arrow) as efferent limb
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


