Case presentation
A 12-year-old male presents after a direct fall onto his right arm and shoulder while playing soccer. He is comfortable and prefers to hold the arm close to his body and is supporting the injured arm with his opposite hand. There is an obvious bulge at the midshaft of the clavicle with no abrasion or breaks in the skin seen. There is no tenting of the skin.
Imaging considerations
Plain radiography is the imaging modality of choice in children with suspected clavicle fractures. These fractures can readily be seen on a shoulder series or a chest x-ray. A shoulder series is sufficient if there is no concern for associate pulmonary injury. If there is concern for accompanying thoracic injury, then plain chest radiography should be obtained.
Plain radiography
A single anteroposterior (AP) view is usually sufficient to diagnose most midshaft clavicle fractures and define the angle of displacement. The AP cephalic tilt view (angled 15–45 degrees) is often used in conjunction with the standard AP view to project the clavicle above the ribs, facilitating visualization of fractures and associated displacement. Oblique clavicle views may be added when trying to distinguish between an acromioclavicular (AC) joint injury and a fracture to the distal clavicle, or when the medial clavicle is of greater concern.
Computed tomography (CT)
CT scan is rarely needed for most clavicle fractures. However, medial clavicle fractures and sternoclavicular joint disruption can be missed on plain radiography and CT may be warranted to detect these injuries, as well as to evaluate for other major thoracic injuries in these cases. In select cases where accurate measurement of shortening may influence the decision of operative management, CT scan may be used but should be balanced with the risk for exposure to ionizing radiation in a young patient.
Ultrasound (US)
A small pediatric study showed that bedside US had high positive and negative predictive values (95% and 96%) without any added pain or discomfort when compared to plain radiographs for clavicle fractures. In resource-limited settings, this may be an accurate modality to confirm the diagnosis when clinical suspicion is high and providers have sufficient training in performing musculoskeletal US.
Imaging findings
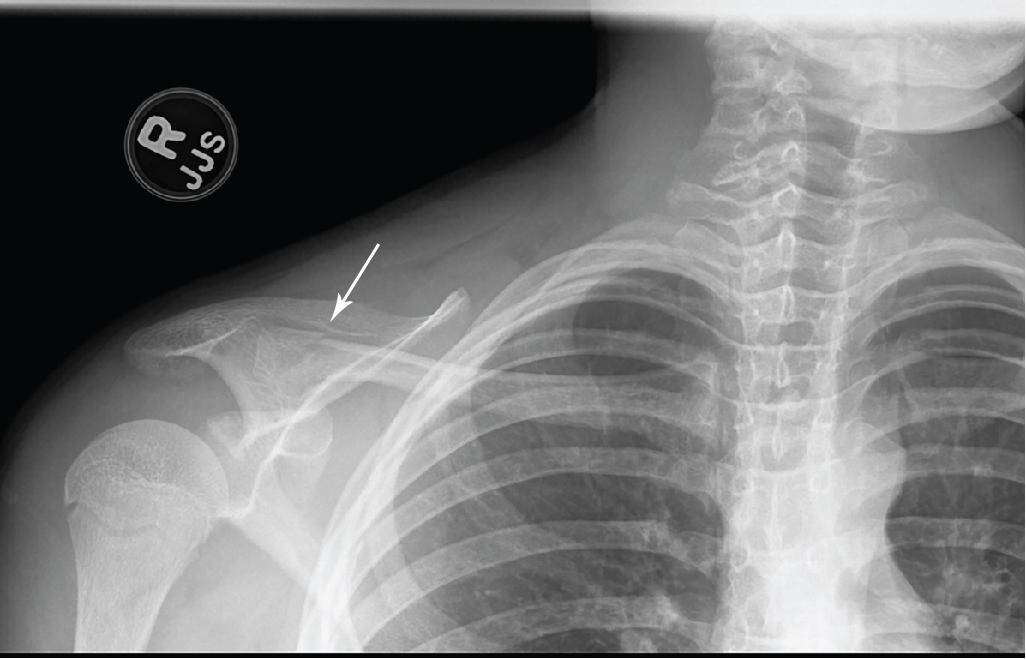
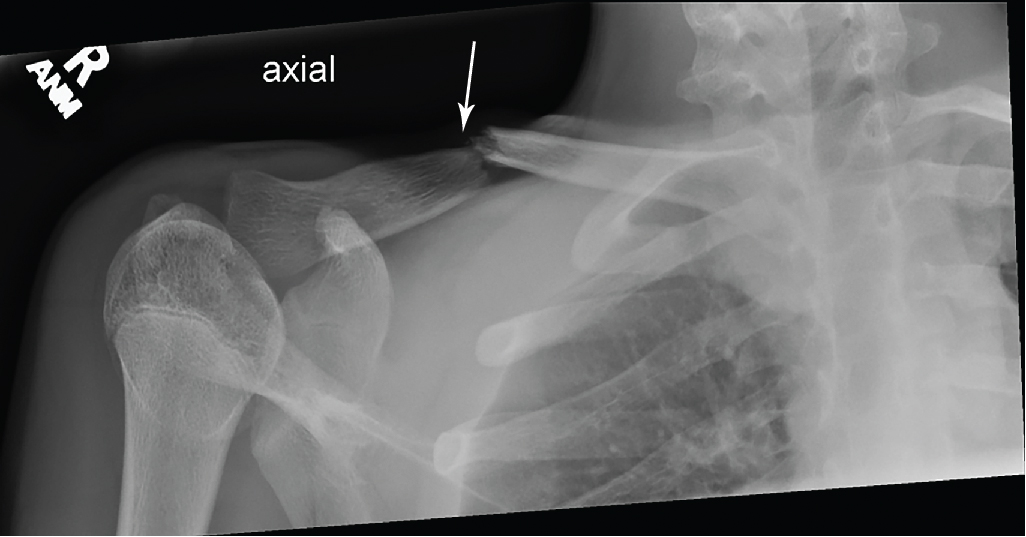
Selected clavicle images for this child are provided. There is an acute, transverse fracture of the mid clavicle, with mild inferior displacement of the distal fracture fragment, with only minimal superior angulation of the fracture apex ( Fig. 56.1 ). An image of the healing fracture, with callus formation, is shown in Fig. 56.2 ; this is the fracture 3 weeks later.
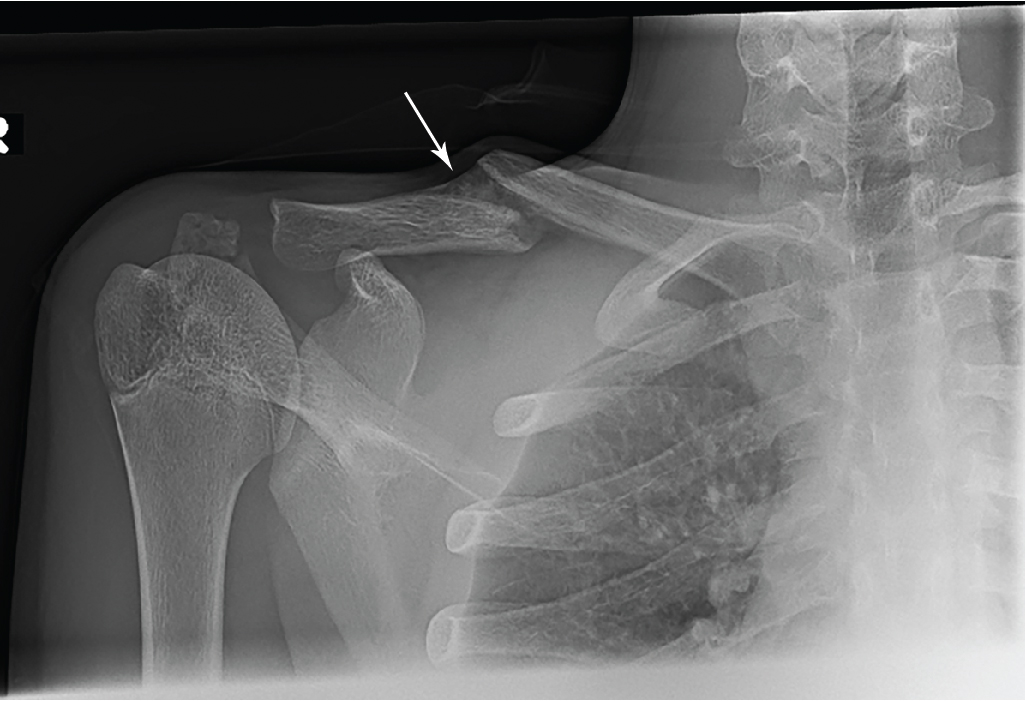
For comparison, Fig. 56.3 shows a distal clavicle fracture from another child. There is an oblique nondisplaced fracture of the lateral right clavicle, just medial to the AC joint.