be a heterogeneous autoimmune disorder, with genetic factors playing an important role in the disease expression. Although the association with the susceptibility loci of HLA-DRB1 and PTPN22 genes is best understood, several non-HLA loci have been linked to this arthritis, including the 18q21 chromosome region of the TNFRSR11A gene, which encodes the receptor activator of nuclear factor κB. In addition, a common genetic variant at the TRAF1-C5 locus on chromosome 9 is associated with an increased risk of anti-CCP-positive rheumatoid arthritis. The detection of rheumatoid factor, representing specific antibodies in the patient’s serum, is an important diagnostic finding. Although it is still debatable, some investigators also include under this rubric a condition called seronegative rheumatoid arthritis (see later), in which patients present without rheumatoid factor but with the clinical and radiographic picture of rheumatoid arthritis.
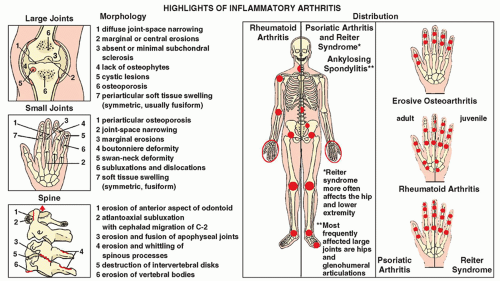 FIGURE 14.1 Inflammatory arthritides. Highlights of the morphology and distribution of arthritic lesions in the inflammatory arthritides. |
TABLE 14.1 Clinical and Imaging Hallmarks of Inflammatory Arthritides | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
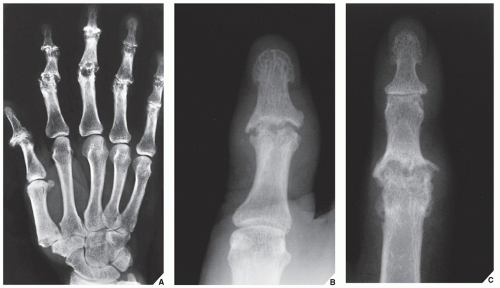 FIGURE 14.2 Erosive osteoarthritis. (A) Dorsovolar film of the left hand of a 48-year-old woman with erosive osteoarthritis shows the typical involvement of the proximal and distal interphalangeal joints. Note the “gull-wing” pattern of articular erosion, a configuration resulting from peripheral bone erosion in the distal side of the joint and central erosion in the proximal side of the joint associated with marginal bone proliferation. (B) Dorsovolar radiograph of the left thumb of a 51-year-old woman shows characteristic gull-wing erosion of the interphalangeal joint. Note adjacent fusiform soft-tissue swelling and lack of periarticular osteoporosis. (C) In another patient, a 50-year-old woman, gull-wing erosion is accompanied by periosteal reaction and fusiform soft-tissue swelling, very similar to psoriatic arthritis. |
 FIGURE 14.3 Progression of erosive osteoarthritis into rheumatoid arthritis. (A) Dorsovolar radiograph of the hand of a 58-year-old woman demonstrates the gull-wing configuration of erosive changes in the proximal interphalangeal joints and the distal interphalangeal joint of the small finger. Because of protracted pain and lack of response to conservative treatment, she underwent joint resection followed by implantation of silicone-rubber prostheses in the proximal interphalangeal joints of the index, middle, and ring fingers, together with fusion of the interphalangeal joint of the thumb and the distal interphalangeal joint of the small finger. Five years after surgery, the classic radiographic features of rheumatoid arthritis developed, involving the wrists (B), elbows, shoulders, hips, and cervical spine. Note the surgical fusion of interphalangeal joints of the thumb and fifth finger as well as the spontaneous fusion of the distal interphalangeal joints of the index and ring fingers. |
 FIGURE 14.4 Rheumatoid arthritis. Anteroposterior (A) and lateral (B) radiographs of the knee of a 52-year-old woman with rheumatoid arthritis affecting several joints show tricompartmental involvement. Note the periarticular osteoporosis, joint effusion, and lack of osteophytosis. |
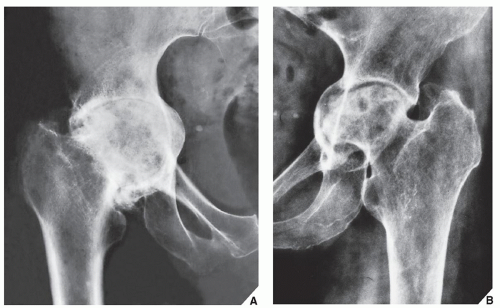 FIGURE 14.5 Rheumatoid arthritis. (A) Anteroposterior radiograph of the right hip of a 60-year-old woman with advanced rheumatoid arthritis shows concentric joint space narrowing, with axial migration of the femoral head leading to acetabular protrusio. Some superimposed secondary osteoarthritic changes are also present. (B) Anteroposterior radiograph of the left hip of a 64-year-old woman shows erosions of the femoral head and acetabulum, concentric narrowing of the hip joint, and acetabular protrusio. |
 FIGURE 14.6 Rheumatoid arthritis. Anteroposterior radiograph of the right shoulder of a 72-year-old man with advanced rheumatoid arthritis shows upward migration of the humeral head secondary to rotator cuff tear, a common complication of rheumatoid changes in the shoulder joint. Note the characteristic tapered erosion of the distal end of the clavicle, erosions of the humeral head, and the substantial degree of periarticular osteoporosis. |
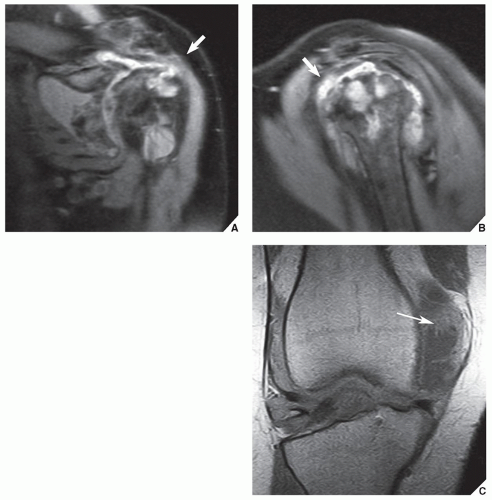 FIGURE 14.7 MRI of rheumatoid arthritis. (A) Oblique coronal and (B) sagittal proton density-weighted fat-suppressed MR images of the left shoulder of a 64-year-old woman show large articular and periarticular erosions, joint space narrowing, joint effusion, and a tear of the supra-spinatus tendon (arrows), all features of advanced rheumatoid arthritis. (C) Coronal T1-weighted MRI of the right knee in another patient demonstrates a joint effusion with inflammatory pannus (arrow). Note the lower signal intensity of the fluid as compared to the slightly higher signal of the pannus. |
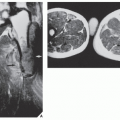
they also may be seen in seronegative inflammatory arthritis and even in tuberculous arthritis. These particles contain collagen, fibrinogen, fibrin, reticulin, elastin, mononuclear cells, blood cells, and some amorphous material. On radiography (Fig. 14.11), this condition occasionally can be mistaken for synovial chondromatosis (see Chapter 23). On MR T1-weighted images, rice bodies exhibit intermediate signal intensity, whereas on T2 weighting, they are only slightly hyperintense relative to muscle (Fig. 14.12).
 FIGURE 14.8 Rheumatoid arthritis. Anteroposterior radiograph of the left hip of a 59-year-old woman with advanced rheumatoid polyarthritis demonstrates the typical erosions of the femoral head and acetabulum. Note the lack of osteophytosis and the only very minimal reactive sclerosis. |
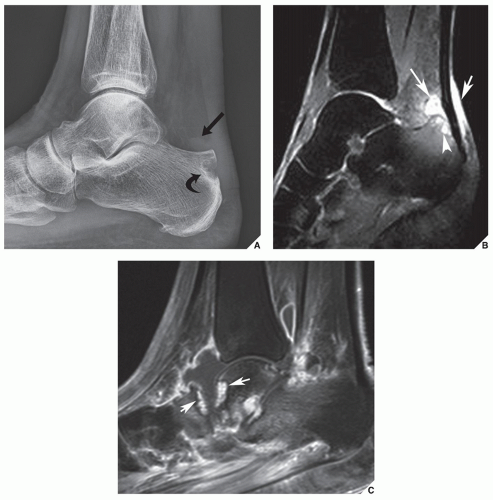 FIGURE 14.9 Rheumatoid arthritis: osseous erosions. (A) Lateral radiograph of the foot of a 55-year-old woman who presented with a heel pain shows fluid in the retrocalcaneal bursa (arrow) associated with erosion of the calcaneus (curved arrow). (B) Sagittal short time inversion recovery (STIR) MR image in another patient demonstrates bone erosion in the posterior process of the calcaneus (arrowhead) associated with extensive surrounding bone marrow edema and retrocalcaneal and retro-Achilles bursitis (arrows). (C) Sagittal T1-weighted fat-saturated postcontrast MRI of the ankle in another patient demonstrates a large tibiotalar joint effusion with enhancing synovium/pannus. Note the bone erosions in the talus and navicular bones containing enhancing inflammatory pannus (arrows). |
 FIGURE 14.10 Rheumatoid cyst. Anteroposterior radiograph of the left knee of a 35-year-old woman with rheumatoid arthritis shows a large synovial cyst in the proximal tibia. Note also articular erosions and periarticular osteoporosis. |
 FIGURE 14.11 Rice bodies. Anteroposterior radiograph of the right shoulder of a 60-year-old woman with advanced rheumatoid arthritis demonstrates multiple rice bodies within subacromial-subdeltoid bursae complex. |
 FIGURE 14.12 MRI of rice bodies. (A) Oblique coronal proton density-weighted, (B) sagittal proton density-weighted, and (C) oblique coronal T2-weighted fat-suppressed MR images of the left shoulder of a 66-year-old woman with rheumatoid arthritis show numerous rice bodies within the shoulder joint. |
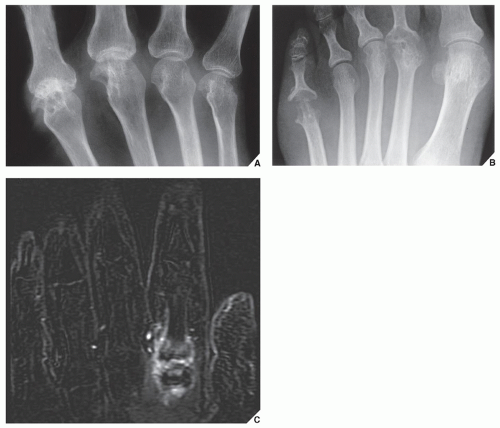 FIGURE 14.13 Rheumatoid arthritis of the small joints. Radiographs of the hand (A) and foot (B) of a 51-year-old woman show typical erosions of the small joints. (C) Coronal STIR MRI in another patient demonstrates bone marrow edema involving the proximal phalanx and distal metacarpal of the second digit, with prominent periarticular soft-tissue edema. Bone marrow edema may be seen on MRI before the bone erosions are seen on radiographs (pre-erosive edema). This feature makes MRI a good tool for establishing an early diagnosis thus leading to early therapy of rheumatoid arthritis. (Courtesy of Luis Cerezal, MD, Santander, Spain). |
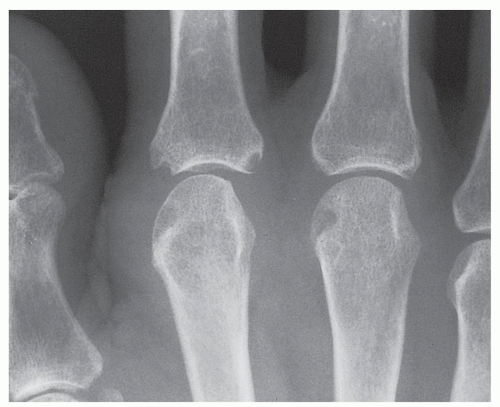 FIGURE 14.14 Rheumatoid arthritis. Typical erosions in the bare areas are seen in this 55-year-old woman with rheumatoid arthritis. Note also periarticular osteoporosis and soft-tissue swelling. |
 FIGURE 14.15 Rheumatoid arthritis. Oblique radiograph of the hand of a 59-year-old woman shows the swan-neck deformity of the second through fifth fingers. Note the flexion in the distal interphalangeal joints and the extension in the proximal interphalangeal joints, the hallmarks of this abnormality. |
 FIGURE 14.16 Rheumatoid arthritis. Dorsovolar radiograph of the hands of a 48-year-old woman demonstrates the boutonnière deformity in the small and ring fingers of the right hand and in the ring finger of the left hand. |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


