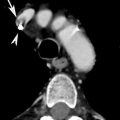
Fig. 1
Thoracic esophageal injury. Water-soluble contrast medium esophagography: leakage of orally administered contrast material (arrow)
In patients with penetrating transmediastinal injury, the most common chest radiographic findings of esophageal perforation are left pleural effusion and cervical or mediastinal soft tissue emphysema. Because the radiographic signs of esophageal injury lack sensitivity and specificity, evaluation with CT, esophagography, or esophagoscopy is necessary (Gunn et al. 2014).
In patients with perforation caused by endoscopy or intubation, chest and lateral neck radiographs may show the presence of linear air collections in the mediastinum, fascial planes of the neck and supraclavicular regions, as well as soft tissue swelling in the retropharyngeal region due to hematoma, edema, or abscess (Ghahremani 1994).
The esophagus is a common site for impaction of foreign bodies that are accidentally or purposefully swallowed. Patients who have esophageal foreign bodies can be classified into four groups: pediatric patients, psychiatric patients and prisoners, patients who have underlying esophageal disease, and edentulous adults (Pinto et al. 2012).
Foreign bodies can sometimes be demonstrated with plain radiographs of the neck or conventional barium esophagogram, but these procedures may fail to show the foreign bodies if they are thin, small, or only faintly radiopaques. Fish bones and chicken bones are the most commonly ingested sharp foreign bodies causing problems in their detection with plain radiographs being obscured by overlying tissues (Pinto et al. 2004).
According to some authors (Flynn et al. 1989), the gold standard for diagnosing an esophageal rupture is iodine, water-soluble contrast medium esophagography, which has a specificity close to 100 % but only a moderate sensitivity of approximately 75 %. In addition to diagnosis, this method helps to determine the location of the perforation but has some disadvantages, such as being operator-dependent and unusable in critically ill patients.
3.2 CT Signs
In patients with clinically suspected esophageal injuries, CT displays the same indirect signs as conventional radiology and more specific signs, such as a localized esophageal wall thickening, mucosal hyperemia, mucosal dissection, an esophageal hematoma, as well as periesophageal air, edema, and fluid (De Lutio di Castelguidone et al. 2005) (Figs. 2, 3, 4, and 5). In patients with suspected perforation caused by foreign body ingestion (Fig. 6), CT can demonstrate such foreign bodies and exhibit superior images compared to plain radiographs, can visualize secondarily induced inflammatory changes in the adjacent structures, and can suggest the site of esophageal perforation.
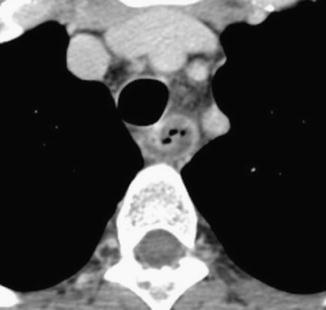
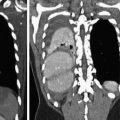
Fig. 2
MDCT demonstrates extensive cervical esophageal wall injury (rectangle) with soft tissues emphysema localized at the level the left submandibular space (arrow) and of the right cervical lateral wall (arrows)
Fig. 3
MDCT examination showing esophageal wall thickening associated with periesophageal edema and fluid (black arrow)
Fig. 4
MDCT demonstrates the presence of periesophageal fluid and small bubble gas
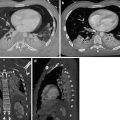
Fig. 5
Perforation of the thoracic esophagus. MDCT shows the presence of pneumomediastinum (a, large arrow), left pleural effusion, periesophageal air (a–d, small arrow), and leakage of orally administered contrast material (c, d, black arrow)
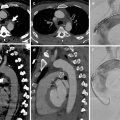
Fig. 6
MDCT shows a foreign body (chicken bone, arrow) impacted at the level of cervical esophagus without signs of esophageal perforation
In cases of traumatic esophageal perforation, MDCT is very useful for detecting the presence of pneumomediastinum, mediastinitis, hydropneumothorax, or leakage of orally administered contrast material (Fig. 5) into the mediastinum or pleural space. Moreover, in cases of injury caused by firearms, at MDCT, air bubbles, bullet fragments, or bone fragments located adjacent to the esophagus in the mediastinum suggest esophageal perforation. Thickening or discontinuity of the esophageal wall and extravasation of oral contrast material into the mediastinum are direct MDCT signs of esophageal perforation that have a higher specificity (Dosios et al. 2000).
Due to particular anatomic direction of the esophagus, multiplanar reformatted images allow a better identification of the extent of perforation and their complications and also the possible involvement of adjacent structures.
4 Management and Treatment
Review of the literature revealed that esophageal perforations are frequently diagnosed late and that the associated mortality is high (Brinster et al. 2004). Early diagnosis reduces mortality. However, suspicion is first necessary for early diagnosis. When esophageal rupture is suspected, diagnosis is often determined with contrast esophagography, chest radiograph, MDCT, or upper gastrointestinal system endoscopy.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


